
To the Editor:
Pheochromocytoma presents with headache, sweating, and palpitations associated with hypertension, heart failure, and arrhythmias due to catecholamine secretion.1 The presence of sustained ventricular tachycardia (VT) has been reported rarely.2,3 We describe a case of pheochromocytoma that manifested as sustained and incessant monomorphic VT.
A 47-year-old woman with diabetes and hypertension under therapy, who had experienced episodes of back pain, palpitations, and dyspnea from 5 months earlier, was seen in the emergency room during an episode. Blood pressure was 130/65 mm Hg and troponin T 0.30 ng/mL (normal <0.01), with normal creatine kinase and myoglobin. The baseline electrocardiogram was normal (Figure 1). However, during follow-up, the patient presented sustained and incessant runs of ordinary tachycardia with a QRS complex of 0.11 s at 180 bpm, pattern of right bundle-branch block and inferior axis, and atrioventricular dissociation (Figure 2), that reproduced the symptoms. The echocardiography showed left ventricular concentric hypertrophy with normal systolic function; the coronary angiography was normal. Based on the typical pattern of left fascicular origin, intravenous and oral verapamil was administered, stabilizing the sinus rhythm. Monitoring during hospitalization showed episodes of atrial tachycardia with a narrow QRS complex, with heart rates around 150 bpm and persistent sinus tachycardia. Syncopal symptoms were associated with a systolic blood pressure of 240 mm Hg, which dropped to 70 mm Hg within a few minutes without treatment. Thyroid hormone and TSH concentrations were normal, but urinary metanephrines were high. Computed tomography showed a right adrenal mass with a diameter of 6 cm; metaiodobenzylguanidine scintigraphy showed uptake by the mass. Phenoxybenzamine and atenolol therapy stabilized the blood pressure and prevented recurrence of ventricular and atrial tachycardia. A unilateral adrenalectomy was performed, with the diagnosis of pheochromocytoma confirmed by histology. Following surgery, the hypertension was controlled and urinary metanephrines were normalized. Two years after surgery, the patient remained asymptomatic, with no recurrence of arrhythmia and with normal blood pressure.

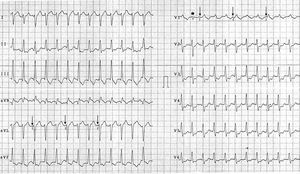
Figure 1. Baseline 12-lead electrocardiogram with a QRS complex pattern and normal repolarization.

Figure 2. Twelve-lead electrocardiogram showing tachycardia, with right bundle-branch block pattern, inferior axis, and QRS complex of 0.11 s. Note the presence of a premature and early narrow QRS complex (*) and atrioventricular dissociation (↓) indicative of ventricular origin.
The most common cardiologic manifestations of pheochromocytoma are heart failure and myocarditis or dilated cardiomyopathy. Ventricular tachycardia has been described in case studies,2-6 and there are no data on the mechanism of this tachycardia, although torsade de pointes has occasionally been reported in relation to a long QT interval.2,4 In our case, the QTC interval was normal and the tachycardia pattern indicated a fascicular origin, but the association with atrial tachycardia pointed to a systemic arrhythmogenic factor. Elevated catecholamines may cause abnormal sinoatrial node pacemaker activity and/or triggering focal activity, and the suppression of pheochromocytoma arrhythmias with alpha and beta blockers5,6 shows the arrhythmogenic role of catecholamines. Verapamil, which should not usually be administered for the treatment of wide QRS complex tachycardia, was used in this patient, following consultation with the arrhythmia specialist, as the pattern clearly indicated a fascicular origin, in the presence of normal ventricular function. The efficacy of verapamil may support an abnormal sinoatrial node pacemaker activity mechanism dependent on Ca++ channels. Adenosine could also be effective for this mechanism,7 but would not be indicated in incessant VT, due to its fleeting effects.
This case shows the importance of a broad differential diagnosis, when the clinical presentation is unusual. The presence of incessant VT of fascicular appearance could have led to "focal" ablation with a catheter, but this would not have detained the systemic arrythmogenic mechanism and would not have cured the symptoms or prevented the potential onset of other foci of tachycardia. The association of frequent crises of atrial tachycardia and inappropriate sinus tachycardia plus sudden changes of blood pressure will guide the diagnosis and allow complete resolution of symptoms following resection of the pheochromocytoma.
A.P. Magalhaes got a grant from Fundación Miguel Servet. Medtronic Ibérica, SA.