
Keywords
INTRODUCTION
Primary cardiac tumors, a rare entity with an incidence of 0.2% in routine autopsies, are benign in 90% of cases. Among the malignant tumors, angiosarcoma is one of the most frequent. Despite the poor prognosis of this disease, surgery is considered the best treatment for patients without distant metastasis. At times, however, radical surgery may be difficult due to local extension of the tumor, the anatomic location or the need for a complex surgical approach. The incidence of recurrence and metastasis is considerable and the highest published survival rates are around 2 years. We describe a patient with primary cardiac angiosarcoma who had undergone surgery on 2 occasions and survived to 4 years, an unusually long period among the published cases.
CASE STUDY
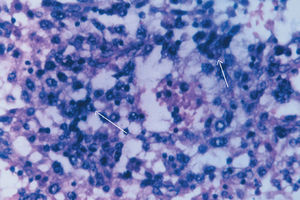
A 57-year-old woman underwent emergency surgery for acute pulmonary edema. Transthoracic echocardiography showed a left atrial mass that protruded through the mitral valve during diastole. The patient underwent surgery with a preoperative diagnosis of left atrial (LA) myxoma. A 6x5x3-cm mass with a 1-cm implantation base extending toward the right inferior pulmonary vein was resected from the posterior wall of the LA. The pathological study indicated angiosarcoma with no infiltration at the borders (Figure 1).

Figure 1. Histological study showing atypical endothelial cells diagnosed as angiosarcoma (hematoxylin and eosin stain, x40).
The extension study using computed tomography (CT), brain magnetic resonance imaging (MRI), cardiac resonance, and bone scintigraphy study showed no metastasis. The patient was subsequently treated with 6 cycles of chemotherapy consisting of ifosfamide, adriamycin, and methotrexate, and was discharged in partial remission.
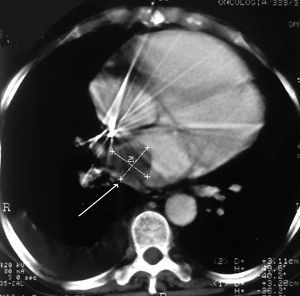
Two years later, the patient came to the emergency room for an episode of atrial fibrillation. Transthoracic echocardiography and CT (Figure 2) disclosed a large left atrial mass, unaffected pulmonary veins and a severe double mitral lesion. The patient's functional class deteriorated and a new extension study was negative for metastasis. A second surgical procedure was undertaken to remove the mass, which extended from the posterior LA wall to the right inferior pulmonary vein and affected the posterior mitral valve (Figure 3). The posterior LA wall and part of the posterior mitral valve were resected and reconstructed with a bovine pericardium patch.

Figure 2. Chest CT showing a hypodense area corresponding to the tumor mass located in the left atrium.

Figure 3. Tumor mass affecting the mitral valve (second surgery).
The patient received another six cycles of chemotherapy (adriamycin, ifosfamide). Two years after the second surgery, the patient died of multiorgan failure after local and distant recurrence of the tumor.
DISCUSSION
Primary cardiac tumors are rare, with an incidence ranging from 0.0017% to 0.003%, depending on the series.1 Among the malignant tumors, sarcomas are the most frequent (76%-78%) and angiosarcoma accounts for about 31% of all primary cardiac malignant tumors.1 With the advances in echocardiography, CT and MRI, more cases of this disease are being diagnosed before surgery. However, in many patients the diagnosis is not established until after pathological examination of the surgical specimen. The prognosis is poor and the mean survival is usually 6 to 11 months from the time of diagnosis.2 Survival up to 3 years has been reported in a few cases,2,3 however, the correlation study showed that histological grade is not an independent factor related with survival in cardiac sarcomas.3 It does appear that tumors located in the left heart have a better prognosis.3 Nevertheless, aggressive resection with reconstruction associated with chemotherapy and valve repair or replacement when necessary have indisputably been shown to improve survival among these patients.4
Some authors have proposed orthotopic heart transplantation as a surgical alternative. However, except for sporadic cases in which the histological type was not angiosarcoma, the published survival data do not differ from those obtained with conventional surgery5 (6-66 months). Autografts, which would theoretically offer better access to the tumor and therefore greater possibilities for resection and reconstruction of cardiac structures,5 present similar results.
In conclusion, we suggest that surgery associated with new drugs from the therapeutic armamentarium for cancer patients may significantly prolong life among patients with malignant primary cardiac tumors. In any case, when adequate surgical treatment is offered, patients can benefit from a better quality of life during the survival period.
Correspondence: Dra. T. Centella Hernández.
Servicio de Cirugía Cardíaca de Adultos. Hospital Ramón y Cajal.
Carretera de Colmenar, km. 9,100. 28034 Madrid. España.
E-mail: centellato@teleline.es