
Transcatheter aortic valve replacement (TAVR) is an expanding technique, and increasing numbers of patients are carriers of transcatheter aortic heart valves (TAHV). Previous instances of TAHV dysfunction have been documented, mostly due to progressive aortic regurgitation (AR) or acute AR as a result of iatrogenesis or endocarditis. These cases have been successfully treated with TAVR. In this report, we present a case whose peculiarity lies in its acute presentation due to leaflet rupture, with no apparent cause, and its successful treatment with redo-TAVR. The patient provided consent for this communication.
An 85-year-old woman was admitted to the cardiovascular intensive care unit due to acute heart failure, low blood pressure, and elevated levels of troponin T and NT-proBNP (peak 538 pg/mL and 3,974 pg/mL, respectively). Electrocardiogram only revealed signs of left ventricular overload. The patient had a history of hypertension, obesity, mild thrombocytopenia, secondary hyperparathyroidism, and chronic gastritis. Six years prior, she had undergone TAVR, with a coronary angiogram showing normal coronary arteries. The implanted prosthesis was a 29-mm CoreValve Evolut PRO (Medtronic, United States) and subsequent echocardiographic follow-up showed no signs of dysfunction.
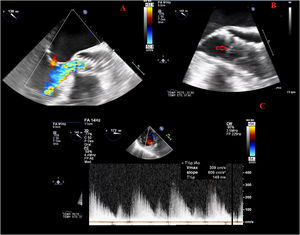
However, due to onset of acute heart failure, transthoracic echocardiography (TTE) was performed and a severe intraprosthetic AR jet was observed, which occupied the entire area of the prosthesis, despite preserved ejection fraction. Following clinical stabilization, a TEE was performed (figure 1A-C, and videos 1 and 2 of the supplementary data). Severe intraprosthetic AR was confirmed with a pressure half-time of 149 ms and a jet width that spanned the entirety of the left ventricular outflow tract. This phenomenon was attributed to the detachment of the theoretically noncoronary leaflet.
. Transcatheter aortic valve with severe AR jet occupying the entire LVOT. B: TEE LVOT midesophageal view. The transcatheter valve can be visualized, and the arrow points to an uninserted leaflet that suggests leaflet rupture. C: Doppler continuous TEE image. Transgastric transverse view of the AR jet. AR, aortic regurgitation; LVOT, left ventricle outflow tract; TEE, transesophageal echocardiography.")
A: color Doppler TEE (midesophageal view in LVOT). Transcatheter aortic valve with severe AR jet occupying the entire LVOT. B: TEE LVOT midesophageal view. The transcatheter valve can be visualized, and the arrow points to an uninserted leaflet that suggests leaflet rupture. C: Doppler continuous TEE image. Transgastric transverse view of the AR jet. AR, aortic regurgitation; LVOT, left ventricle outflow tract; TEE, transesophageal echocardiography.
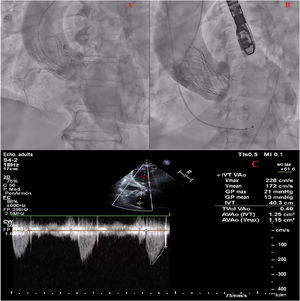
During admission, no fever or clinical or laboratory signs suggestive of systemic infection were evident. The patient had undergone a TTE 6 months prior, which had indicated a normally functioning prosthesis without AR and she had not previously consulted for heart failure symptoms. To rule out endocarditis, both blood and urine cultures were obtained, with negative results. Coronary angiography (figure 2A and video 3 of the supplementary data) revealed unobstructed coronary arteries and severe AR. The elevation in troponin T elevation appeared to be a consequence of acute heart failure and shock.

A: contrast angiogram of the ascending aorta. Transcatheter aortic valve with severe AR that fills the entire LV with contrast. B: contrast angiogram at the end of redo-TAVR without residual AR. C: Doppler continuous transthoracic echocardiography. Absence of AR and valve-in-valve gradients within the normal range. AR, aortic regurgitation; LV, Left ventricle; TAVR, transcatheter aortic valve replacement.
Heart Team decided on valve intervention by redo-TAVR. Since the aortic contrast angiogram showed a low risk of coronary occlusion or sinus of Valsalva sequestration, the decision was made not to perform computed tomography prior to the procedure. This decision aimed prevent overloading the patient with contrast and to avoid any potential delays to the procedure due to the clinical situation.
During admission, the procedure was performed, with implantation of a 29-mm CoreValve Evolut PRO self-expanding prosthesis by direct implantation 3mm below the previous prosthesis (video 4 of the supplementary data), through right femoral access in conjunction with left radial access. Femoral closure was performed with 3 suture-mediated vascular closure devices. The absence of AR was verified by angiography (figure 2B and video 4 of the supplementary data) and by TEE.
After the procedure, the patient remained in the cardiovascular intensive care unit for 48hours, with no complications. Prior to discharge, a follow-up TTE was performed (figure 2C), verifying normal functioning of the prosthesis and the absence of AR. At 3 months, the patient was asymptomatic and a follow-up TTE showed normal functioning of the prosthesis.
Currently, TAVR has become the treatment of choice for severe aortic stenosis in patients at high surgical risk1 and is increasingly used in the low surgical risk population. In addition, the procedure has also been used as a treatment for surgical bioprosthesis dysfunction with similar results to redo surgical aortic valve replacement in high-risk patients.2 TAHV dysfunction has been less frequently described than bioprostheses dysfunction. However, because of the increase in its prevalence and its use in an increasingly younger population, there is a need for data on the long-term durability of transcatheter prostheses and for strategies to treat their eventual failure. Registries report that the main cause of TAHV dysfunction is AR. They are generally cases of progressive presentation and those with acute forms are usually of clear etiology or valve-in-valve.3,4
The peculiarity of our case is the acute presentation of severe AR due to leaflet rupture in a TAHV implanted 6 years previously, with no apparent cause (no fever and negative blood cultures, in addition to TEE without images suggestive of endocarditis). This is a case of valve structural deterioration according to the definition of the European consensus of valve failure in bioprosthesis.5 Being a high-risk surgical patient, the chosen option for treatment was redo-TAVR. The absence of computed tomography images was a limitation for the choice of the prosthesis and the planning of the procedure.
In the registry by Landes et al.6 on redo-TAVR, 1-year survival was 88%, with few periprocedural complications. Reviewing the available literature, we have only found 1 similar case4 in a patient with a previous redo-TAVR, who showed acute dysfunction of the prosthesis and was treated with surgical aortic valve replacement, but we have found no cases of acute dysfunction of a TAHV due to spontaneous leaflet rupture treated by redo-TAVR.
In conclusion, acute TAHV dysfunction with severe AR due to spontaneous leaflet rupture is rare but possible and is an emergency that can be effectively treated by redo-TAVR.
FUNDINGNone.
AUTHORS’ CONTRIBUTIONSÁ. Pinar Abellán wrote and designed the text and figures. M. López Vázquez and N. Vallejo Calcerrada reviewed and edited the article. A. Gallardo López, J. Jiménez Mazuecos, and D. Melehi El Assali participated in the interventional procedures and reviewed the article.
CONFLICTS OF INTERESTThe authors have no conflicts of interest to declare.