
Diet is part of the secondary prevention treatment in patients with coronary artery disease (CAD). The guidelines of American societies usually recommend following a diet that is low in saturated fats, whereas European guidelines also include adopting eating habits based on the Mediterranean diet (MedD); however, this diet is only referred to explicitly in the National Institute for Clinical Excellence (NICE) guidelines.
Recently, the PREDIMED1 study, conducted amongst the Spanish population without coronary disease but at high cardiovascular risk, showed the superior efficacy of the MedD supplemented with virgin olive oil or nuts and dried fruit versus a low-fat diet against cardiovascular morbidity and mortality. In this study, the 14-point Mediterranean diet adherence screener (MEDAS–14) was validated, and a good correlation was shown between proper adherence to the diet and its efficacy.2 In secondary prevention, the Lyon Diet Heart Study3 demonstrated the benefit of a diet that closely followed the MedD in reducing reinfarction and clinical manifestations of CAD. Studies conducted in patient cohorts who had suffered acute coronary syndrome observed clinical benefits associated with greater adherence to the MedD, including a reduction in total mortality4.
We decided to investigate MedD adherence by CAD patients seen at a primary care center, using the MEDAS–14 screener.
We studied 110 patients selected from the total number of patients seen at the primary care centre, aged between 55 and 80 years, who were diagnosed with CAD, in ascending order starting from the oldest diagnostic coding date. Institutionalised patients and patients with health problems that could shorten their life expectancy or who were incapable of answering a questionnaire were excluded. The patients answered the MEDAS–14 screener and completed the data collection protocol, which included sociodemographic variables, domestic habits, physical activity, cardiovascular risk factors, and prescription of cardioprotective drugs.
Eighty per cent were retired males and 60% performed nonintensive regular exercise 3 or more days per week. The principal characteristics of the series are listed in the Table. The mean score on the screener was 8.9 points (scale from 0 to 14), and ≥ 9 points (acceptable adherence criterion) in 63% (95% confidence interval, 54%-72%). Adherence to each of the 14 points of the screener is shown in the Figure. Compared with studies in which the same screener was used, the mean score was similar to the baseline score of the PREDIMED1 study and higher than that of general population surveys.5 The percentage of patients with acceptable adherence (63% with a score ≥ 9) was also higher compared with the general population,5 but similar to the baseline of the PREDIMED study, 54%. We did not find any studies in the literature that used MEDAS–14 to screen patients with CAD. We believe it is reasonable for CAD patients to show greater adherence, particularly if the disease is relatively recent, as they would probably be more receptive to an educational intervention to promote the uptake of heart-healthy habits than the general population or patients at low risk.
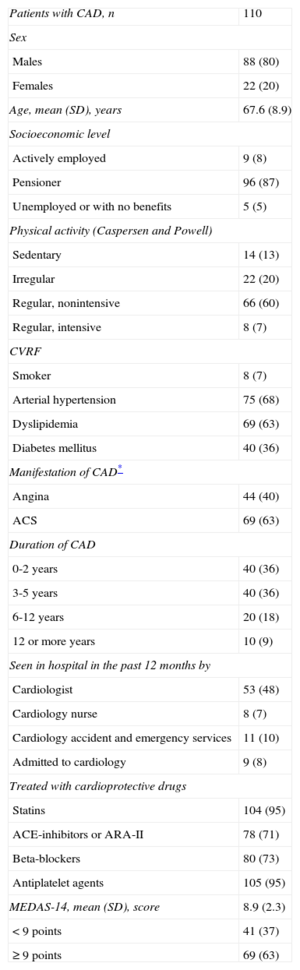
Principal Characteristics of Patients Diagnosed With Coronary Artery Disease Who Answered the MEDAS–14 Screener
| Patients with CAD, n | 110 |
| Sex | |
| Males | 88 (80) |
| Females | 22 (20) |
| Age, mean (SD), years | 67.6 (8.9) |
| Socioeconomic level | |
| Actively employed | 9 (8) |
| Pensioner | 96 (87) |
| Unemployed or with no benefits | 5 (5) |
| Physical activity (Caspersen and Powell) | |
| Sedentary | 14 (13) |
| Irregular | 22 (20) |
| Regular, nonintensive | 66 (60) |
| Regular, intensive | 8 (7) |
| CVRF | |
| Smoker | 8 (7) |
| Arterial hypertension | 75 (68) |
| Dyslipidemia | 69 (63) |
| Diabetes mellitus | 40 (36) |
| Manifestation of CAD* | |
| Angina | 44 (40) |
| ACS | 69 (63) |
| Duration of CAD | |
| 0-2 years | 40 (36) |
| 3-5 years | 40 (36) |
| 6-12 years | 20 (18) |
| 12 or more years | 10 (9) |
| Seen in hospital in the past 12 months by | |
| Cardiologist | 53 (48) |
| Cardiology nurse | 8 (7) |
| Cardiology accident and emergency services | 11 (10) |
| Admitted to cardiology | 9 (8) |
| Treated with cardioprotective drugs | |
| Statins | 104 (95) |
| ACE-inhibitors or ARA-II | 78 (71) |
| Beta-blockers | 80 (73) |
| Antiplatelet agents | 105 (95) |
| MEDAS-14, mean (SD), score | 8.9 (2.3) |
| < 9 points | 41 (37) |
| ≥ 9 points | 69 (63) |
ACE-inhibitors, angiotensin converting enzyme inhibitors; ACS, acute coronary syndrome; ARA–II, angiotensin II receptor antagonist; CAD, coronary artery disease; CVRF, cardiovascular risk factors; MEDAS-14, 14-point mediterranean diet adherence screener.
Identifying the screener items that are not fully met is just as valuable as determining the degree of adherence. According to the recommendations, these include insufficient consumption of wine, fruit, pulses, vegetables and nuts or dried fruits, and olive oil should certainly be added too (Figure).
 of the 110 patients with coronary artery disease. 95%CI, 95% confidence interval.")
The general recommendation of restricting, for example, the ingestion of fruit in diabetics, alcohol in hypertensive patients or pulses, or oil and nuts or dried fruit in obese patients may have influenced the results. In order to improve adherence, each item of the MedD should be examined in detail and recommendations should be tailored to each patient's circumstances.
With regard to the established recommendations, the knowledge provided by the PREDIMED study is of particular interest, as it highlights the additional consumption of extra virgin olive oil and nuts or dried fruit, together with the increased adherence to the MedD, as key elements for the superior efficacy of this diet compared with a low-fat diet.
It is likely that the MedD will be clearly reinforced as an intervention to be included in nonpharmacological treatment for preventing cardiovascular disease,6 thanks to the possibility of new studies backing the results published by de Lorgeril et al.3
The data from this study show that a majority of patients with CAD (63%) had acceptable adherence to the MedD. The application of the MEDAS–14 screener makes it possible to identify which aspects require improvement and provides the opportunity to focus and adapt a dietary intervention.
Pere Roura Poch, biostatistician at the Unitat de Suport a la Recerca de la Gerencia Territorial de la Catalunya Central, for his cooperation and comments.