
Heart failure (HF) has been considered to be the great cardiovascular”epidemic“of the 21st century due to its high and increasing incidence and prevalence as well as its high mortality.1,2 One of the consequences of the enormous magnitude and severity of HF is the large number of hospital admissions, which are frequent despite treatment and lead to worsening prognosis, deterioration in the quality of life of patients and caregivers, and a high economic burden on the health care system.2,3 Indeed, several studies have shown that the admissions rate for HF in Spain since the 1990s has been steadily increasing4 and that this trend has continued in the early years of 21st century.5,6 The RECALCAR study of the Spanish Society of Cardiology6 has shown that one of the main reasons for the increasing incidence of HF admissions is population aging.
To further investigate this trend in Spain and the influence of advanced age on the number of HF hospitalizations, we studied the prevalence of admissions for HF episodes in Spanish Health Care System (HCS) hospitals. The data source was the minimum data set (MBDS) of the Ministry of Health. We selected all admissions of patients with a main diagnosis of HF between January 1, 2006 and December 31, 2019. These episodes were coded according to the International Classification of Diseases (ICD-9 until 2015; ICD-10 from 2016 onward).
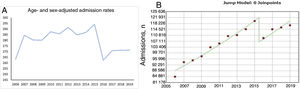
From 2006 to 2009, there were 371 566 admissions for HF in Spanish HCS hospitals. However, from 2016 to 2019, there were 456 461 admissions, representing a significant increase of 22.8% (P <.001) despite underreporting in 2016 due to changes in the coding system. Nevertheless, when adjusted for age and sex (direct method), the admission rate (age- and sex-adjusted admissions per 100 000 population) was lower from 2017 to 2019 than from 2006 to 2015 (271 vs 286; P <.001). From 2006 to 2019, the percentage of patients aged at least 75 years admitted for HF significantly increased vs all HF admissions (from 69.9% in 2007 to 77.5% in 2019 [P <.001]). The number of admissions in this age group also significantly increased from 262 629 (2006-2009) to 351 589 (2016-2019). Indeed, this 33.8% increase was larger than the increase in total HF admissions (22.8%). Table 1 shows the trend (2006-2019) in the number of HF admissions, the age- and sex-adjusted rate of admissions per 100 000 population, the number and percentage of admissions of patients aged at least 75 years, and the number of admissions and age- and sex-adjusted rates of men and women aged at least 75 years. The overall incidence rate ratio is shown and also for the periods 2006 to 2015 and 2017 to 2019. Although there was an increasing trend in the number of admissions for HF, it can be seen that, from 2006 to 2019, the age- and sex-adjusted admission rate tended to decrease (IRR,0.98; 95% confidence interval [95%CI], 0.98-0.99; P <.001) and then flattened from 2017 to 2019 (IRR,1; 95%CI, 1-1; P <.001) (figure 1A). However, in that period, there was a significant increase in the number and percentage of HF admissions of patients aged at least 75 years (table 1). Table 1 also shows a decrease in HF admissions between 2015 and 2016, which was due to changes in the MDS coding system (ICD-9 until 2015; ICD-10 from 2016 onward). However, the slope representing the increase in the number of admissions remained similar before and after the change in coding (see figure 1B, joinpoint model).
Number of total HF admissions, age- and sex-adjusted admission rates per 100 000 population, and admissions and percentage of admissions of HF patients aged at least 75 years in Spain from 2006 to 2019.
| Year | Total admissions for HF | Admission ratea | Admissions for HF, age ≥75 y | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | Men | Men, age-adjusted | Women | Women, age-adjusted | Age-and sex-adjusted | |||
| 2006 | 84 881 | 263.2 | 57 948 | 68.3 | 22 371 | 1708 | 35 574 | 1681 | 1691 |
| 2007 | 93 972 | 284.5 | 65 655 | 69.9 | 25 248 | 1850 | 40 406 | 1843 | 1845 |
| 2008 | 95 073 | 280.3 | 67 997 | 71.5 | 26 590 | 1868 | 41 406 | 1823 | 1840 |
| 2009 | 97 640 | 280.1 | 71 029 | 72.7 | 27 823 | 1880 | 43 204 | 1842 | 1856 |
| 2010 | 103 305 | 287.6 | 76 330 | 73.9 | 30 124 | 1960 | 46 205 | 1906 | 1926 |
| 2011 | 105 674 | 285.7 | 79 334 | 75.1 | 31 406 | 1969 | 47 936 | 1914 | 1935 |
| 2012 | 110 318 | 291.4 | 83 900 | 76.1 | 33 277 | 2031 | 50 622 | 1977 | 1997 |
| 2013 | 110 937 | 284.9 | 84 611 | 76.3 | 34 521 | 2055 | 50 090 | 1913 | 1967 |
| 2014 | 114 626 | 286.9 | 87 362 | 76.2 | 35 063 | 2057 | 52 298 | 1968 | 2001 |
| 2015 | 119 775 | 294.1 | 91 046 | 76.3 | 37 059 | 2135 | 54 347 | 2017 | 2062 |
| 2016b | 109 088 | 262.4 | 83 674 | 76.7 | 33 898 | 1904 | 49 773 | 1813 | 1848 |
| 2017 | 114 571 | 270.8 | 87 961 | 76.8 | 36 075 | 1995 | 51 885 | 1864 | 1914 |
| 2018 | 115 735 | 271.2 | 89 174 | 77.1 | 36 581 | 2000 | 52 591 | 1880 | 1926 |
| 2019 | 117 068 | 271.3 | 90 780 | 77.5 | 37 247 | 2004 | 53 533 | 1894 | 1936 |
| Total | 1 492 663 | 280.2 | 1 117 171 | 74.8 | 447 283 | 1972 | 669 870 | 1890 | 1921 |
| IRR (95%CI) | 1.02 (1.02-1.03) | 0.98 (0.98-0.99) | 1.03 (1.02-1.04) | 1.01 (1.01-1.01) | 1.03 (1.03-1.04) | 1.00 (1.00-1.01) | 1.03 (1.02-1.03) | 1.00 (1.00-1.01) | 1.01 (1.00-1.01) |
| P | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | .030 |
| IRR (95%CI), 2006-2015 | 1.03 (1.03-1.04) | 1.00 (1.00-1.01) | 1.04 (1.04-1.05) | 1.01 (1.01-1.01) | 1.05 (1.05-1.06) | 1.02 (1.02-1.03) | 1.04 (1.03-1.05) | 1.02 (1.01-1.02) | 1.01 (1.00-1.02) |
| P | <.001 | .007 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | .026 |
| IRR (95% CI), 2017-2019 | 1.01 (1.01-1.01) | 1.00 (1.00-1.00) | 1.02 (1.01-1.02) | 1.00 (1.00-1.00) | 1.01 (1.01-1.02) | 1.00 (1.00-1.003) | 1.02 (1.01-1.02) | 1.01 (1.00-1.00) | 1.00 (1.00-1.00) |
| P | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 | <.001 |
HF, heart failure; 95%CI, 95% confidence interval; IRR, incidence rate ratio.
; from 2017 onward, it remains at 271/100 000 population. B: joinpoint model of the number of admissions from 2006 to 2019; there was a decrease of 12.78% per year from 2015 to 2016. The annual percentage change and average annual percentage change are significant and equal (3.4), indicating that the trend did not change.")
A: trend in the adjusted admission rates of patients aged at least 75 years admitted for heart failure. In 2016, the age- and sex-adjusted admission rate decreased (underreporting); from 2017 onward, it remains at 271/100 000 population. B: joinpoint model of the number of admissions from 2006 to 2019; there was a decrease of 12.78% per year from 2015 to 2016. The annual percentage change and average annual percentage change are significant and equal (3.4), indicating that the trend did not change.
These results suggest 2 main points: a) in Spain, the age- and sex-adjusted admissions rate per 100 000 population has recently decreased; this is the first time this trend has been observed; and b) the percentage of admissions among patients aged at least 75 years has continued to increase. Therefore, it could be said that admissions for HF in Spain have stabilized, especially in patients younger than 75 years. This result could be related to advances in the treatment of HF, improvements in the organization of care management due to the implementation of HF programs, or a shift in the disease to older ages due to improvements in the health determinants of Spanish citizens. However, the HF”epidemic” continues to be of immense concern and places a huge burden on the Spanish HCS, especially because of the large population of older people in Spain.
FUNDINGThis study was conducted with the help of an unconditional grant from Menarini (SEC RECALCAR Project). Menarini has not participated in any part of the preparation and submission process.
AUTHORS’ CONTRIBUTIONSAll the authors participated equally in the conception, design, analysis, writing, and revision of the article.
CONFLICTS OF INTERESTNone declared.
We would like to thank the Ministry of Health for its help in developing the RECALCAR project, with special thanks to the Instituto de Información Sanitaria.