


Ischemic heart disease is the leading cause of death and one of the top 4 causes of burden of disease worldwide. The aim of this study was to evaluate age-period-cohort effects on mortality from ischemic heart disease in Andalusia (southern Spain) and in each of its 8 provinces during the period 1981-2008.
MethodsA population-based ecological study was conducted. In all, 145 539 deaths from ischemic heart disease were analyzed for individuals aged between 30 and 84 years who died in Andalusia in the study period. A nonlinear regression model was estimated for each sex and geographical area using spline functions.
ResultsThere was an upward trend in male and female mortality rate by age from the age of 30 years. The risk of death for men and women showed a downward trend for cohorts born after 1920, decreasing after 1960 with a steep slope among men. Analysis of the period effect showed that male and female death risk first remained steady from 1981 to 1990 and then increased between 1990 and 2000, only to decrease again until 2008.
ConclusionsThere were similar age-period-cohort effects on mortality in all the provinces of Andalusia and for Andalusia as a whole. If the observed cohort and period effects persist, male and female mortality from ischemic heart disease will continue to decline.
Keywords
Ischemic heart disease is the leading cause of death and is one of the top 4 causes of burden of disease worldwide. More than 7 millions deaths are produced annually, accounting for around 13% of all deaths.1,2 Additionally, ischemic heart disease is now responsible for 5.8% of years of life lost due to premature mortality.3–5
Death rates from ischemic heart disease have diminished considerably over the last few decades in Europe and other continents in response to improvements in health promotion policies, health care, and treatments.6–8 As in other European Union countries, the trend in Spain is toward declining male and female mortality. The crude rate was 7.5 deaths per 10 000 population in 2011 (8.6 for men and 6.3 for women), making ischemic heart disease the first cause of death among men and the second among women.9,10 These figures mean that Spain is currently one of the European Union countries with the lowest mortality from ischemic heart disease.8 However, as Spanish statistics tend to vary by region, proper health planning requires analysis of regional mortality patterns.11
Andalusia (southern Spain) accounts for 18% of the Spanish population.9,12 It is the most highly populated autonomous community in Spain. Administratively it is divided into the 8 provinces of Almeria, Cadiz, Cordoba, Granada, Huelva, Jaen, Malaga, and Seville (Figure 1). According to the latest official figures, the crude death rate from ischemic heart disease in Andalusia was 7.9 per 10 000 population in 2011 (8.9 for males and 6.9 for females).10,13
 and its administrative division into 8 provinces.")
The Interactive Mortality Atlas for Andalusia was implemented in Andalusia for epidemiological surveillance purposes.14 Analyses of the annually updated Interactive Mortality Atlas for Andalusia data provide insights into the geographical distribution of mortality from ischemic heart disease over time in southern Spain. Recent studies based on these data show that currently, in over 95% of the Andalusian municipalities, male and female mortality rates for age groups under 65 years are similar to, or significantly lower than, the corresponding Spanish rates. Since 1981, however, male and female mortality rates for age groups older than 65 years have been significantly higher in the western Andalusia region. As is the case with other municipalities and other causes of death, the ischemic heart disease mortality rate ratio in age groups older than 65 years has generally been falling in this region since 2000, and the death rate is tending to gradually reduce the significant difference with the Spanish figure.15,16
These results suggest a possible age-period-cohort effect on mortality from ischemic heart disease, with higher mortality observed compared with previous years, possibly because of certain features of past periods and generations that have gradually disappeared from the newer population cohorts.
Age-period-cohort analyses are typically performed using pooled time-period data and 5-year age groups. Because this approach to aggregation can result in significant bias in estimating trends, recent studies suggest that time-based analyses of mortality rates should minimize confusion between age, death period, and birth cohort by using data tabulated for periods as small as possible and by treating age, period and cohort as continuous variables.17 This would result in more accurate results, even though the complexity of the mathematical models used is greater.
The aim of this study was to evaluate the effect of birth cohort, adjusted by the year of death and age, on male and female deaths from ischemic heart disease in Andalusia as a whole and in each of its 8 provinces during the period 1981 to 2008, using continuous-time statistical models.
METHODSDesignAn ecological study was implemented with a Lexis diagram triangle comprising each annual age group, year of death, and year of birth as the unit of analysis.
ScopeThe study was conducted in Andalusia as a whole and in each of its 8 provinces.
PopulationIn all, 145 539 deaths from ischemic heart disease (ICD-9 [ninth revision of the International Classification of Diseases] 410-414 and ICD-10 [tenth revision of the International Classification of Diseases] I20-I25), 90 387 in males and 55 152 in females, were analyzed for individuals between the ages of 30 and 84 years who died in Andalusia in the period 1981 to 2008. The deaths correspond, therefore, to cohorts born between 1896 and 1978.
VariablesUsing information recorded for each death (the person's age, sex, year of birth, year of death, and province of residence), the number of male and female deaths in each province was compiled and grouped by 1-year age, year of death, and year of birth. The number of male and female inhabitants for each province was also recorded, grouped by 1-year age and year of death.
Information SourcesMortality data were obtained from the Andalusian Institute of Statistics and Cartography, via the General Secretariat of Public Health and Participation (Secretaría General de Salud Pública y Participación) attached to the Department of Health (Consejería de Salud) of the Autonomous Government of Andalusia (Junta de Andalucía). Population data were obtained from the Spanish National Institute of Statistics for the period 1981 to 2002 and from municipal registries for the period 2003 to 2008.
Statistical AnalysisA Lexis diagram tabulating deaths and person-years by age, period, and cohort was used for the statistical analysis of the data. Because age, period, and cohort are originally continuous variables, their impact on the death rate was analyzed in a continuous-time model, which allowed us to calculate the death rate at any point in the Lexis diagram.17 A nonlinear regression model was estimated for each sex and geographical area, with the mortality rate observed for each age, year of death, and birth cohort as the dependent variable. The formulation of the multiplicative age–period–cohort model for rate r(a, p) at age a in period p for persons in birth cohort c = p – a is:

This is a usual approach to modelling effects, where fa, gp and hc are respectively the age, period, and cohort functions. To obtain identifiability, hc was restricted to be 0 for the reference cohort c0=1932 (an intermediate point for the cohorts born between 1896 and 1978 that has been previously used in other age-period-cohort analyses in Andalusia), and gp was constrained to be 0 on average and to have 0 slope on the logarithmic scale. Thus, fa is interpretable as log age-specific rates in the reference cohort after adjustment for the period effect, hc is the log relative risk relative to cohort c0, and gp is the residual log relative risk, ie, log relative risk relative to the age-cohort prediction. Each term was parameterized using natural splines functions with 7 knots.17,18
The linear trend (drift) was extracted from the model using the Holford method. This parameter represents the overall slope of the time trend due to both cohort and period.17
The analysis was implemented in R programming language using the apc.fit function from the Epi package.19 Separate analyses were performed for each sex, for each province and for Andalusia as a whole.
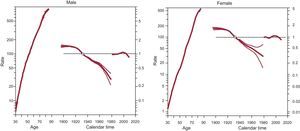
RESULTSResults are described in terms of trend charts obtained for each age-period-cohort model. Each graph has 3 curves depicting, from left to right, trends in mortality rate by age for the reference cohort, mortality risk by birth cohort (taking 1932 as the reference), and mortality risk by year of death (taking the mortality average of the period as the reference). The horizontal axis of the graph is divided in 2 parts: 1 for age (years-old) and 1 for cohort-period (calendar years). The left vertical axis represents mortality rates for the age effect and the right vertical axis represents relative risk for the cohort and period effects. A dot has been placed at (1932, 1) to indicate the reference cohort.
Age EffectThere was an upward trend in male and female mortality by age for Andalusia as a whole from the age of 30 years (Figure 2). A similar trend was observed for all the provinces (Figures 3–4).

Age-period-cohort effects, with its corresponding confidence intervals, on mortality from ischemic heart disease in Andalusia as a whole. Each graph has 3 curves depicting, from left to right, death rates per 100 000 population by age for the reference cohort, relative risk of mortality by birth cohort and relative risk of mortality by calendar year.

Age-period-cohort effects, with its corresponding confidence intervals, on male mortality from ischemic heart disease in the provinces of Andalusia. Each graph has 3 curves depicting, from left to right, death rates per 100 000 population by age for the reference cohort, relative risk of mortality by birth cohort and relative risk of mortality by calendar year.

Age-period-cohort effects, with its corresponding confidence intervals, on female mortality from ischemic heart disease in the provinces of Andalusia. Each graph has 3 curves depicting, from left to right, death rates per 100 000 population by age for the reference cohort, relative risk of mortality by birth cohort and relative risk of mortality by calendar year.
In Andalusia, the risk of death for men and women remained steady for cohorts born between 1896 and 1920. From 1920, the male and female risk showed a downward trend, decreasing after 1960 with a steep slope among men (Figure 2).
The male and female mortality trends by birth cohort were similar for Andalusia as a whole as well as for each of its provinces, with the exception of Jaen and Malaga. These provinces experienced a steady increase in male and female mortality risk for cohorts born after 1960 (Figures 3–4). However, the small number of deaths from ischemic heart disease registered for the most recent cohorts and the width of the confidence intervals suggest that these were not statistically significant increases.
Period-of-death EffectThe death risk for men and women in Andalusia first remained steady from 1981 to 1990 and then increased between 1990 and 2000, only to decrease again until the end of the study period (Figure 2). This pattern was, moreover, replicated in each of the Andalusian provinces, with the exception of Jaen, Almeria, and Huelva. These provinces experienced a more oscillating mortality trend either for men or for women (Figures 3–4).
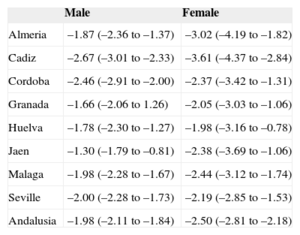
Overall, the estimated annual decrease in Andalusian mortality rates was −1.98% for men and −2.50% for women (Table). These linear changes were statistically significant for both male and female mortality. Similar results were observed for all the provinces of Andalusia. Cadiz was the province that showed the highest annual decrease in mortality rates for men (–2.67%) and women (–3.61%) (Table).
Annual Percent Change in Mortality Risk from Ischemic Heart Disease in Andalusia
| Male | Female | |
|---|---|---|
| Almeria | –1.87 (–2.36 to –1.37) | –3.02 (–4.19 to –1.82) |
| Cadiz | –2.67 (–3.01 to –2.33) | –3.61 (–4.37 to –2.84) |
| Cordoba | –2.46 (–2.91 to –2.00) | –2.37 (–3.42 to –1.31) |
| Granada | –1.66 (–2.06 to 1.26) | –2.05 (–3.03 to –1.06) |
| Huelva | –1.78 (–2.30 to –1.27) | –1.98 (–3.16 to –0.78) |
| Jaen | –1.30 (–1.79 to –0.81) | –2.38 (–3.69 to –1.06) |
| Malaga | –1.98 (–2.28 to –1.67) | –2.44 (–3.12 to –1.74) |
| Seville | –2.00 (–2.28 to –1.73) | –2.19 (–2.85 to –1.53) |
| Andalusia | –1.98 (–2.11 to –1.84) | –2.50 (–2.81 to –2.18) |
Linear trend (drift) of the percentages of variation, with the 95% confidence interval in parentheses.
This study points to an age-period-cohort effect on mortality from ischemic heart disease that was similar in all the geographical areas studied.
Age EffectThe results showed a progressive increase in male and female death rates with age. These findings are in line with other studies performed around the world, which have also shown that men have a higher death rate than women at all ages, regardless of income or development levels.8
Age is one of the main nonmodifiable risk factors for ischemic heart disease. Moreover, aging is related to a higher probability of having high blood pressure, diabetes mellitus and hypercholesterolemia and of being inactive, as well as other modifiable risk factors.20Overall, hypertension and diabetes mellitus are 2 of the most important risk factors for ischemic heart disease in people of all ages and is the major risk factor in the elderly.4,21–23 In Spain and Andalusia, the prevalence of both hypertension and diabetes mellitus increased with age.24–26The prevalence of hypertension is currently 72% among Spaniards older than 65 years, and the prevalence of diabetes mellitus is 29% among men and 24% among women.27 These figures could explain the steady rise in the death rate with age found in this study and corroborates the findings of other Spanish studies.28
Birth Cohort EffectFor Andalusia as a whole and for each of its provinces, the analysis of the cohort effect revealed a steady fall in the mortality risk from ischemic heart disease for all generations born after 1920. This finding has also been observed in previous Spanish and worldwide studies, suggesting that the continuous advances in medical technology and healthcare could explain the steady fall in the risk of mortality in developed countries.29,30 Indeed, Spain has undergone a remarkable social and economic transformation since the beginning of the 20th century, which has favored improvement in treatments and healthcare for ischemic heart disease and in health promotion for successive generations.31,32 In addition, the Mediterranean diet and the progressive improvements in nutrition of Spanish generations have led to cardiovascular benefits, which could have contributed to reducing the risk of death.33,34 In fact, Spain is now one of the European Union countries with the lowest mortality from ischemic heart disease.7,8
Smoking is an important modifiable risk factor for ischemic heart disease. In Spain and Andalusia, the prevalence of tobacco consumption has progressively declined in males born after 1950. In contrast, the prevalence of daily tobacco consumption has increased steadily among women born after 1930, and especially for post-1960 generations.35,36 This could be related to the steeper slope of the risk of death for post-1960 male generations in Andalusia, which was not observed among women born after 1960.
Recent studies worldwide have found an effect of birth cohort on the prevalence of obesity, diabetes mellitus and other modifiable risk factors for ischemic heart disease, suggesting that cohort-specific strategies may be needed to combat the high prevalence of risk factors and to reduce their impact on mortality.37–41 Unfortunately, there are no similar studies in Andalusia that support this hypothesis. However, nutritional excesses in more recent Spanish generations have begun to fuel infant obesity and other health problems that could change the future trend in the risk of mortality from ischemic heart disease in Andalusia.42
Period-of-death EffectThe period effect showed an oscillating mortality trend, which first remained steady from 1981 to 1990, then increased between 1990 and 2000, and finally decreased again until 2008.
Healthcare reform in Andalusia lasted into the 1990s, following Spanish Government devolution to Andalusia of the responsibility for healthcare. The increase of the death risk before this reform is compatible with the late effects of cumulative exposure to tobacco smoking, environmental and occupational exposures, lack of sufficient healthcare or efficient diagnostic procedures, and scarce preventive and therapeutic procedures during that period in Andalusia and in Spain as a whole.43 In addition, there is evidence that the prevalence of obesity, hypertension, and hypercholesterolemia started to increase in adults in the 1990s.44–46 Because all of these factors are modifiable risk factors for ischemic heart disease, the upwards trends in the prevalence could be related to the increasing trend in the mortality risk during the last decade of the 20th century. Today, the prevalence of obesity continues to increase in Andalusia. For this reason, health promotion policies should be implemented to control the overweight epidemic and, as a result, to reduce the incidence of ischemic heart disease and associated mortality.26
On analyzing the specific causes of death, it was seen that the International Classification of Diseases code changes implemented with ICD-10 in 1999 may have affected the mortality trends. These changes, however, did not affect mortality from ischemic heart disease in Spain.47,48 Therefore, the explanation for the decline in trend for the period 2000-2008 must be related to other factors.
After the healthcare reform in Andalusia, health promotion and disease prevention measures were gradually introduced, as well as advances in medical technology.49 Thus, the treatment of patients with high blood pressure changed from 5% in 1980 to 20% in 2002, and a similar increase was observed in the treatment of hypercholesterolemia.50 In 1994, the Department of Health of the Autonomous Government of Andalusia created the EPES (Empresa Pública de Emergencias Sanitarias). The number of patients treated by this service increased progressively from 17 500 in 1995 to 60 000 in 2008, and the new therapies, such as prehospital fibrinolytic therapy, increased from 18% in 2000 to 30% in 2005. A clear reduction in intrahospital mortality was also reported for this period.51,52 In addition, heart rehabilitation units were widely implemented in 1997, contributing to improved quality of life and survival. This, together with the generalization of angioplasty after 1998, was related to a subsequent reduction in mortality from acute myocardial infarction.28,53,54Around 2000, the Department of Health of the Autonomous Government of Andalusia started the I Health Care Quality Program, which has led to continuous quality improvement and the standardization of procedures based on clinical evidence for the effective management of cardiovascular events and other diseases. In 2005, the Comprehensive Care Plan for Heart Disease was implemented in Andalusia, with the aim of enhancing knowledge of heart disease and of promoting heart-healthy lifestyles.55All these actions, taken together, have increased the quality of healthcare provision and improved treatments, with a consequent increase in survival and reduction in deaths from ischemic heart disease, as has occurred in Spain as a whole during the first decade of the 21th century.11,49
Recent studies have shown that half of the decrease in mortality from coronary heart disease in Spain is attributable to evidence-based therapies, and half to reductions in the main modifiable risk factors.43 Since the end of the 1990s, the prevalence of high blood pressure, dyslipidemia, diabetes mellitus, and female smoking has increased in Andalusia, making it one of the Spanish regions with the highest prevalence of cardiovascular risk factors.26,27,44 However, the incidence of ischemic heart disease has remained relatively stable since 2000.26 These findings suggest that the declining mortality for the period 2000-2008 may be principally due to improved health policies, treatment, and patient care. In addition, because the main reduction in risk factors is still to be produced, as a result of the Integrated Health Plans implemented by the Department of Health of the Autonomous Government of Andalusia in 2005, the decline of mortality may accelerate in the next few years.56,57
CONCLUSIONSAge-period-cohort effects on mortality from ischemic heart disease were similar in all the provinces of Andalusia and for Andalusia as a whole. The cohort effect showed a steady fall in the mortality risk for male and female generations born after 1920. The period effect revealed a reversal in male and female mortality trends, which decreases declines since 2000. These results could explain the higher mortality from ischemic heart disease observed in the past in the provinces of Cadiz, Huelva and Seville (western Andalusia region) for age groups older than 65 years, as well as the subsequent fall in mortality since the mid-1990s.15 In fact, in this study, Cadiz was the province with highest annual decrease in male and female mortality rates.
If the observed cohort and period effects persist, mortality from ischemic heart disease will continue to decline for males and females. However, the steady increase in the main modifiable risk factors in Andalusia could change future mortality trends. For this reason, health promotion policies should continue to control the overweight epidemic and other relevant risk factors. In addition, the implementation of new treatments, as well as novel healthcare policies that improve the care of ischemic heart disease should be promoted.
CONFLICTS OF INTERESTNone declared.