Keywords
INTRODUCTION
Hypothyroidism can lead to well-known and classic cardiovascular abnormalities such as a reduced cardiac output, arterial hypertension, sinus bradycardia, prolonged QT interval, and pericardial effusion. Hypothyroid cardiomyopathy is an uncommon manifestation of hypothyroidism that can take the form of dilated cardiomyopathy1,2 or, more unusually, asymmetric septal hypertrophy. This latter condition was first described in 1980 by Santos et al.3 Here, we present the case of a patient with primary hypothyroidism who was being treated by hormone-replacement therapy and who presented with a relapse characterized by myxedema and global myocardial hypertrophy, predominantly septal, that remitted after the patient attained an euthyroid state.
CASE REPORT
A 61-year-old woman was admitted with symptoms of severe asthenia and anorexia of several weeks of duration. There were no specific symptoms of heart failure. During the previous 48 hours, these symptoms had been accompanied by fever and joint pain. Her medical history included arterial hypertension, depression, and regular constipation. She had undergone three cesarean sections and had been diagnosed with hypothyroidism 20 years previously. Since then, she had been treated with L-thyroxine, 100 μg/day. At the last check-up, 2 years previously, her thyroid function was normal.
Physical examination showed slight obesity, cold sallow skin, and pallor, but no goiter. The remainder of her physical examination was normal: temperature, 35.5°C; arterial pressure, 120/80 mm Hg, and heart rate, 80 beats/min.
Laboratory studies showed: hemoglobin, 11.6 g/dL; mean corpuscular volume, 78 fL; mean corpuscular hemoglobin, 26 pg; total cholesterol, 148 mg/dL (high-density lipoprotein cholesterol, 23 mg/dL; low-density lipoprotein cholesterol, 58 mg/dL), and triglycerides, 333 mg/dL. Iron metabolism studies gave normal results and arterial gas measurements were normal. In addition, the total protein level was 5.2 g/dL and the albumin level was slightly below normal, at 47.3%. Other measurements were: creatine kinase, 286 U/L (normal values: under 180 U/L); creatine kinase MB fraction, 26 U/L; sodium, 127 mEq/L; thyrotropin (thyroid-stimulating hormone or TSH), 23.52 U/mL (normal values: 0.304.20 U/mL); and free thyroxine (T4), 1.11 ng/dL (normal values: 0.90-1.70 ng/dL). Testing for antithyroid antibodies was negative.
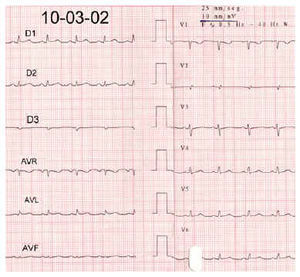
An electrocardiogram (ECG) demonstrated sinus rhythm and there was a general reduction in voltage level (Figure 1). Chest radiography revealed slight cardiomegaly. Transthoracic echocardiography detected generalized hypertrophy of both ventricles, with a septal thickness of 18 mm and a left ventricular posterior wall thickness of 15 mm. There was no outflow obstruction. In addition, the myocardium had a hyperdense mottled appearance. Both the ejection fraction and mitral filling rate indicated normal systolic and diastolic function (Figure 2). Abdominal echocardiography showed only hepatic steatosis. A rectal biopsy was carried out but no amyloid deposits were found.

Fig. 1. Initial electrocardiogram showing sinus rhythm and a general reduction in the voltage level of the QRS complex.

Fig. 2. Transthoracic echocardiography showing global parietal hypertrophy of both ventricles, predominantly septal (thickness, 18 mm), with a posterior wall thickness of 15 mm. Upper image: apical 4-chamber view. Lower image: M-mode scan, parasternal long axis view.
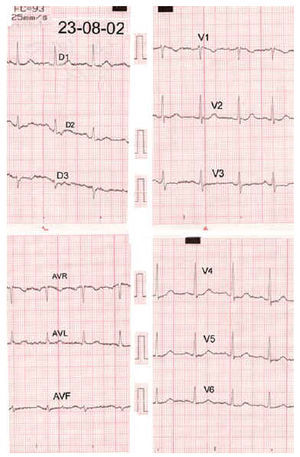
After the L-thyroxine dose was increased to 125 μg/day, the patient experienced a general improvement in her symptoms of asthenia and anorexia, and laboratory results also improved. Hormone measurements carried out 3 months after admission were normal: TSH, 0.19 U/mL, and free T4, 1.29 ng/dL. An ECG made 5 months after discharge showed clear changes, with a recovery in the voltage level in all leads (Figure 3). In the 2 echocardiography check-ups carried out within the 2 years following admission, it was possible to observe regression of the ventricular hypertrophy, with normalization of the myocardial thickness. However, a slight hyperdense mottle appearance remained (Figure 4).

Fig. 3. Electrocardiogram made after the patient returned to a euthyroid state, showing normalization of the QRS-complex voltage level.

Fig. 4. Transthoracic echocardiography carried out 2 years after the patient returned to a euthyroid state. The upper and lower views are the same as those in Figure 2.
Clinical, electrocardiographic and echocardiographic observations in our patient suggested a diagnosis of hypothyroid cardiomyopathy that manifested as reversible asymmetric septal hypertrophy.
DISCUSSION
Here, we have described the case of a patient with primary hypothyroidism who was receiving hormone-replacement therapy and presented with a relapse characterized by myxedema. In this patient, we were able to demonstrate the presence of global myocardial hypertrophy, predominantly septal, which was accompanied by a general reduction in the voltage level of the electrocardiographic QRS complex. These findings returned to normal once the patient achieved a euthyroid state.
Myocardial hypertrophy, manifesting as reversible asymmetric septal hypertrophy, was first described by Santos et al3 in 1980. In their series of 19 patients with myxedema, 17 presented with this type of reversible cardiomyopathy. Since then, seven more publications have been added to the literature,4-10 giving a total of 74 patients, of whom four were children.4,5 Intercellular and intracellular deposition of myxedematous material leads to structural alterations, which partially account for the abnormalities observed on the ECG (i.e., the low signal voltage).11,12
In our patient, the observation of a hormone profile that was characteristic of subclinical hypothyroidism (an elevated TSH level with a T4 level at the lower limit) was paradoxical given the presenting clinical symptoms. To date, only alterations in systolic and diastolic function have been reported in subclinical hypothyroidism; structural alterations in the heart have not.13,14 It is possible that this phenomenon is due to a direct biological effect of TSH, as has been suggested by some authors,14,15 or perhaps the TSH concentration more accurately reflects the actual peripheral level of thyroid hormone activity. Whatever the explanation, it is surprising that a small fluctuation in hormonal state can induce clear clinical manifestations, not least structural alterations in the heart.
We believe this case report is of interest because it is unusual and because it serves as a reminder that there is a form of reversible myocardial hypertrophy that can be caused by hypothyroidism.
Correspondence: Dr. A. Felices Nieto.
Luis Fuentes Bejarano, 3, casa 75. 41020 Sevilla. España.
E-mail: afelices@supercable.es