To the Editor,
Neonatal aortic coarctation is a serious condition. It is characterized by signs of heart failure and cardiogenic shock.
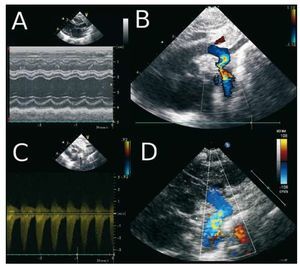
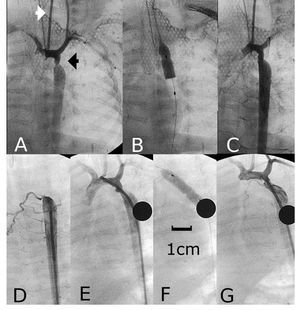
We report the case of a premature twin, born at the gestational age of 32 weeks, with intrauterine growth retardation, referred to our hospital at the age of 17 days with severe heart failure. Echocardiography revealed severe left ventricular dysfunction (Figure 1A); the dimensions of left ventricle in M mode were 19 mm and 13 mm in diastole and systole, respectively. The aortic arch showed severe coarctation (Figure 1B), with a gradient of 40 mmHg diastolic extension (Figure 1C). Treatment was begun with prostaglandin E1, diuretics and inotropic agents. He also required mechanical ventilation. When he was 24 days old and weighed 1200 g, angioplasty was performed using the Seldinger technique, involving a 3-F introducer in the left carotid artery (Figure 2A). The aortic arch, the region of the coarctation and descending aorta measured 3.5 mm, 1.5 mm, and 5 mm in diameter, respectively. A 4 mm ´ 20 mm Tyshak Mini® balloon catheter (NuMED, Hopkinton, NY, USA) (Figure 2B) was utilized. Following angioplasty, the coarcted segment increased in diameter to 4 mm (Figure 2C). The initial gradient of 35 mmHg disappeared completely. The fluoroscopy time was 7 minutes. After the procedure, the administration of prostaglandins and inotropic agents was discontinued. Starting at 30 days of life, a progressive aortic recoarctation was observed, although it was well tolerated clinically. At the age of 61 days, with a body weight of 2200 grams, the infant underwent a second angioplasty procedure with access via the right femoral artery. The angiography revealed severe recoarctation (Figures 2D and 2E); in addition, permeability of the left common carotid artery utilized in the previous procedure was observed (Figure 2E). With the aid of a 4-F introducer, a 5 mm ´ 20 mm Tyshak Mini® balloon catheter was used (Figure 2F), followed by another measuring 6 mm ´ 20 mm. The initial gradient of 40 mmHg was reduced to 7 mmHg. At the age of 6 months, the infant was asymptomatic and showed adequate weight gain, with a body weight of 5600 grams; echocardiography demonstrated the absence of a gradient in the aortic arch, with a normal color flow Doppler ultrasound (Figure 1D).

Figure 1. Echocardiography prior to angioplasty (access via carotid artery). A: M mode, showing left ventricular dysfunction. B: coarcted aortic arch. C: Doppler ultrasound with gradient of 40 mmHg and diastolic extension. D: aortic arch following second angioplasty (at 6 months of age).

Figure 2. A, B, and C: first aortic angioplasty, access via carotid artery. D, E, and F: aortic angioplasty, access via femoral artery: note (E) the permeability of the left carotid artery utilized in the previous procedure.
The treatment of severe coarctation in premature infants requires prolonged infusion of prostaglandins to maintain perfusion in the abdomen and lower extremities.
Both surgery and angioplasty prove to be effective in the treatment of native coarctation, but the latter is associated over the long term with more complications, such as recoarctation and the formation of aneurysms.1
Despite the improvement in the results of the surgical treatment of coarctation, prematurity is perceived as a risk factor for morbidity and mortality; in 2 different studies,2,3 the rate of acute mortality was reported to be 5.5% to 12.5%, whereas late mortality ranged between 8.3% and 11%. Moreover, the authors observed recoarctation in 29% and 44% of the treated patients.
Experience with angioplasty in premature infants is limited. In a review4 dealing with premature infants weighing less than 1500 grams, four of them with coarctation required six procedures, and two had to undergo surgery to treat recoarctation. There was one death that was not related to the procedure. Other articles involve case reports5,6; the smaller of the 2 children described to was a premature infant weighing 460 grams. Both cases were treated successfully, but neither of them involved access via the carotid artery, as we performed in our patient.
Angioplasty in premature infants with aortic coarctation is, in our opinion, a treatment that can improve the serious clinical condition of these patients. We consider that access via the carotid artery not only permits easy vascular access, but is a safe technique as well.