


Carbohydrate antigen 125 (CA125), a biomarker associated with fluid overload, has proven useful in managing diuretic therapy in heart failure. We aimed to evaluate the impact of diuretic optimization guided by CA125 before transcatheter aortic valve implantation (TAVI) on outcomes.
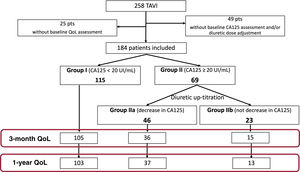
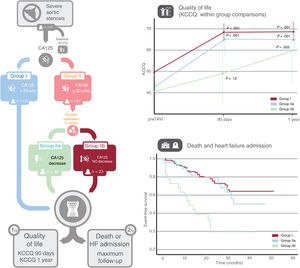
MethodsThis prospective interventional study enrolled patients scheduled for TAVI, in whom baseline CA125 was measured 2 weeks before TAVI. Patients with CA125 ≥ 20 U/mL underwent diuretic up-titration before TAVI. Three groups were included: group I) baseline CA125 <20 U/mL; IIa) CA125 ≥ 20 U/mL that decreased after treatment, and IIb) CA125 ≥ 20 U/mL that did not decrease. The primary outcome was changes in the Kansas City Cardiomyopathy Questionnaire at 3 and 12 months. The secondary endpoint was clinical events.
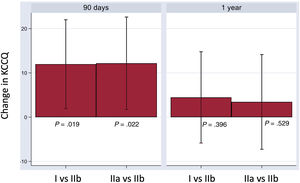
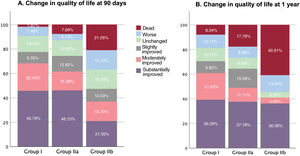
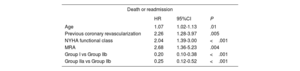
ResultsThe study included 184 patients (115 group I, 46 IIa, and 23 IIb). Groups I and IIa exhibited early and sustained improvements in the Kansas City Cardiomyopathy Questionnaire (group I: 18.9 points [95%CI, 15.7-22.1; P <.001] at 90 days, and 18.1 [95%CI, 14.9-21.4, P <.001] at 1 year; group IIa: 21.1 points [95%CI, 15.4-26.7; P <.001] and 19.5 [95%CI, 13.9-25.1; P <.001] respectively). In contrast, in group IIb there was no significant improvement at 90 days (P=.12), with improvement being significant only at 1 year (17.8 points, 95%CI, 5.9-29.6; P=.003). Over a median follow-up of 20.7 months, there were 63 (27.83%) deaths or heart failure admissions. Multivariate analysis showed a lower risk of events in group I vs IIb (HR, 0.28; 95%CI, 0.14-0.58; P <.001), and IIa vs IIb (HR, 0.24; 95%CI, 0.11-0.55; P <.001).
ConclusionsPatients with persistently high CA125 despite diuretic therapy pre-TAVI showed slower functional recovery and poorer clinical outcomes after TAVI.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm