

In recent years, there has been a notable shift in cardiovascular clinical practice within cardiology and surgery. The CARDIOXCARDIO study aimed to identify professionals’ opinions on working practices and relations between specialties. A survey was simultaneously sent to the 4442 members of the Spanish Society of Cardiovascular and Endovascular Surgery (SECCE) and the Spanish Society of Cardiology (SEC), yielding 385 valid responses. More than half (59%) of respondents were men, mostly specialists (7.3% residents), and 74.8% worked in the field of cardiology, predominantly in public centers (88.3%). Using a Likert scale ranging from 1 to 5 (worst to best), respondents rated relations between surgery and cardiology with an average of 3.57±0.9 points. Cardiologists rated surgeons with a mean score of 3.83±0.8, while surgeons gave cardiologists a mean score of 3,92±0.72. In addition, respondents provided numerous suggestions for improvement, which are discussed in detail, highlighting certain discrepancies in criteria between specialties. Implementing strategies based on the suggestions of professionals, together with a proactive approach to continuous improvement, could substantially enhance the quality of cardiovascular care in Spain.
Keywords
The relationships among the various medical disciplines have been the subject of growing interest in the scientific community, particularly in the field of cardiovascular health.1–4 Both internationally and within Spain, the relations between cardiology and cardiovascular surgery specialties are considered a pivotal area for study and reflection. Cardiology and cardiovascular surgery are crucial branches of cardiovascular medicine that play complementary roles in the prevention, diagnosis, and treatment of cardiac diseases.
The dynamic nature of cardiovascular medicine, marked by technological and scientific advances, has led to a clear and increasingly close interdependence between cardiology and cardiovascular surgery. This evolving relationship has prompted the formation of multidisciplinary Heart Teams.5–7 The need for close collaboration between the professionals of the 2 specialties is driven by the use of cutting-edge technologies, invasive procedures, and innovative therapies, including advances in structural interventional cardiology. This situation has encouraged an integrated focus for addressing the complexity of patients with cardiovascular diseases but may sometimes lead to discord and arguments. As a result, numerous expert and consensus documents now emphasize the need for collaboration between specialties, and specific guidelines have been drafted to support this cooperation.6
In addition, the growing prevalence of cardiac diseases in an ever-aging society with multiple comorbidities has emphasized the importance of fluid cooperation and efficient communication between cardiologists and cardiovascular surgeons. A multidisciplinary approach is needed to respond to the unique challenges posed by population aging, the increased prevalence of cardiovascular risk factors, and the diversity of genetic and ethnic profiles. Accordingly, it is the responsibility of professionals to not only develop and implement solutions for managing patients’ problems, but also to stitch together the resources required to achieve harmonious and optimized multidisciplinary health care. In this context, it is increasingly important to foster smooth logistical and personal relationships. Nonetheless, the collaboration between these 2 specialties is not without challenges and controversies; careful attention should be paid to debates sparked by differences in therapeutic approaches, professional skills, and care models. Based on the above, the steering committees of the Spanish Society of Cardiology (SEC) and the Spanish Society of Cardiovascular and Endovascular Surgery (SECCE) have identified the need to work together in the stated direction.
Accordingly, a joint commission was formed with members of the 2 societies to analyze the current situation and to promote joint ventures.8 This project included the CARDIOXCARDIO study, whose objective was to analyze the current relationships and working methods between the 2 specialties in Spain. The study was based on the perceptions of professional members of the scientific societies and brought together the specialists of each branch. We examined possible solutions and strategies for strengthening collaboration and guaranteeing an integrated and efficient management of patients with cardiovascular disease. A deeper understanding of this interrelationship would not only enrich academic knowledge, but also have major implications for clinical practice, particularly the cardiovascular health of the Spanish population.
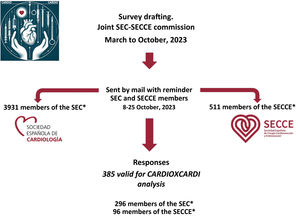
METHODSStudy designThe current work was mainly focused on the working relations and dynamics between cardiology and cardiovascular surgery. A brief voluntary survey was designed (section A of the supplementary data) in electronic format (created using Google Forms) and sent to the 4442 professional members of the SEC and SECCE (figure 1).

The questions were devised by consensus among a group of experts from various disciplines within the 2 societies. The respective society secretaries sent the survey to members with an institutional message endorsed by both societies requesting their participation. Members of both societies may have received 2 copies of the survey. Nonetheless, to avoid duplicates, a single valid response was allowed from each person (judged on an individual basis by using the professional's email address as a key variable).
Quantitative variables (eg, relations, session usefulness) were assessed via scores determined using a Likert scale. Scores were classified from 1 to 5, with 1 always the most unfavorable (eg, “Worst”, “None”) and 5 the most favorable (eg, “Excellent”, “Optimal”, “Extremely useful”). This survey was sent for the first time on October 8, 2023, with a subsequent reminder. The database was closed on October 29, 2023.
EndpointsThe primary endpoint of the CARDIOXCARDIO study was to determine how cardiologists and cardiovascular surgeons of all ages practicing in both publicly funded and private centers in Spain felt about the quality of the working relations and logistics of the 2 specialties. As secondary endpoints, various analyses were conducted by stratifying these opinions based on professional profile (eg, sex, years of experience, discipline).
Finally, we aimed to make some practical recommendations in this field based on the participants’ reflections that could serve as a starting point for joint improvement initiatives. The data obtained in the present work could be useful as a comparative baseline in the coming years. The corresponding database of the present analysis is available for any researcher upon reasonable request.
Statistical analysisIBM SPSS Statistics (version 24; IBM, United States) was used for statistical processing. The study was primarily descriptive. Continuous variables are expressed as mean ± standard deviation and their differences were compared using a t test. Quantitative variables were analyzed using the chi-square test. Hypothesis testing was considered significant with a 2-tailed P value <.05. The statistical treatment and analysis of the results were minimized as much as possible to provide the most descriptive results possible.
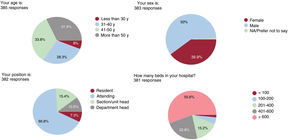
RESULTSDemographic profile of the professionals in the CARDIOXCARDIO sampleIn less than 1 month (from October 9 to October 25, 2023), 385 valid responses were received (8.6% of those surveyed; 18.9% from SECCE members and 7.5% from SEC members). By October 15, 1 week after survey dissemination, 283 responses had been received (73.5% of the total). Of the respondents, 59% were men, and most were specialists with full training (only 7.3% were residents) (figure 2). The age profile indicated that 6% of the participants were aged ≤ 30 years, 28.3% were 31 to 40 years, 33.8% were 41 to 50 years, and 31.9% were older than 50 years. In addition, 50.4% of the professionals had more than 15 years of experience as attending specialists.

Regarding the field of specialty of the sample, the participants were predominantly cardiologists (71.2%) or cardiology residents (3.6%), surgeons (22%), and cardiovascular surgery residents (3.1%). Of the attending cardiologists who responded, 20.4% described themselves mainly as interventional cardiologists, 10.9% as electrophysiologists, 17.3% as imaging specialists, 13.4% as heart failure specialists, and 32.4% as clinicians or cardiac rehabilitation specialists.
Independently of their specialty, 76.6% of participants were SEC members (n=295) while 24.6% were SECCE members (n=96). Overall, 5 (1.3%) did not specify their society and 11 professionals were members of both societies. Most survey respondents (88.3%) worked in publicly funded health centers and 7.8% worked in public-private centers. In addition, 55.6% of respondents worked in centers with more than 600 beds, 38% in centers with 201 to 600 beds, and the remainder in centers with 200 or fewer beds (figure 2). At the time of survey response, 67.6% of participants worked in hospitals with on-site cardiovascular surgery. In contrast, 95% of those without this service stated that they had simple or easy access. For surgical departments, 24.6% conducted more than 500 bypass or major surgeries per year, 63.9% between 101 and 500, and 11.5% 100 or fewer.
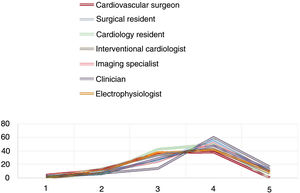
Cardiovascular surgery-cardiology relationsThe survey respondents gave a mean score of 3.57±0.9 to the relations between surgery and cardiology; the scores were 3.64±0.8 for cardiologists and 3.36±0.9 for surgeons (P=.007) (figure 3). Cardiologists rated surgery, as a specialty, with a mean score of 3.83±0.8 while surgeons gave cardiologists a score of 3.92±0.72. The opinions of the professionals regarding their specific center were similar: mean scores of 3.73±1.0 for local surgery and of 3.81±0.8 for local cardiology.
, as well as whether they are resident physicians or not. The numbers on the y-axis show the percentage of participants in each group who assigned that score. The specific score is expressed on the x-axis ranging from 1 to 5, from worst to best.")
Scores given by the participating professionals to the professional relations with their colleagues from the other specialty. The scores are stratified by the cardiology specialty or modality of the professional responding (self-defined), as well as whether they are resident physicians or not. The numbers on the y-axis show the percentage of participants in each group who assigned that score. The specific score is expressed on the x-axis ranging from 1 to 5, from worst to best.
Interventional cardiologists (n=58) rated relations between surgery and cardiology with a mean score of 3.40±0.9. Interventional cardiologists awarded a mean score of 3.3±1.1 to surgeons. Professionals working exclusively in publicly funded centers (the majority [88.1%]) rated relations between surgery and cardiology with a mean score of 3.54±0.9, similar to that of those working in the private system (mean score of 3.87±0.6), and similar to that of professionals working in both systems (mean score of 3.80±0.8).
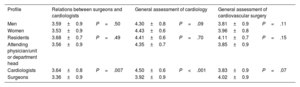
A statistical comparison of groups is shown in table 1. There were no significant differences in the scoring of the cardiology-surgery relationship or in that of cardiology or surgery specialty by age or position (resident or not). However, cardiologists and SEC members gave higher scores. In addition, cardiologists gave a higher score to their specialty than surgeons (P<.001) and vice versa (P=.07).
Analysis of the scores given based on the profile of the professionals who responded
| Profile | Relations between surgeons and cardiologists | General assessment of cardiology | General assessment of cardiovascular surgery | |||
|---|---|---|---|---|---|---|
| Men | 3.59±0.9 | P=.50 | 4.30±0.8 | P=.09 | 3.81±0.9 | P=.11 |
| Women | 3.53±0.9 | 4.43±0.6 | 3.96±0.8 | |||
| Residents | 3.68±0.7 | P=.49 | 4.41±0.6 | P=.70 | 4.11±0.7 | P=.15 |
| Attending physician/unit or department head | 3.56±0.9 | 4.35±0.7 | 3.85±0.9 | |||
| Cardiologists | 3.64±0.8 | P=.007 | 4.50±0.6 | P<.001 | 3.83±0.9 | P=.07 |
| Surgeons | 3.36±0.9 | 3.92±0.9 | 4.02±0.9 | |||
The specific score ranges between 1 and 5, from worst to best, and is expressed as mean±standard deviation. Compared using t test.
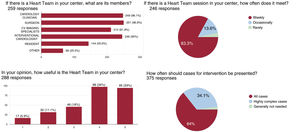
In general, the surveyed professionals assigned a mean score of 3.79±1.1 to medical-surgical sessions. Most respondents reported the existence of these types of sessions in their hospitals (90.6%) and that they were conducted once a week (89.9%). According to the professionals, 66% of these sessions met the criteria of a multidisciplinary team.
Moreover, 64.2% reported the presence of a structured multidisciplinary team in their hospital (59.7% of cardiologists and 77.3% of surgeons; P=.004); these teams mainly comprised clinical cardiology, surgery, and catheterization professionals (figure 4). There were no significant differences between the mean scores of surgeons and cardiologists on the usefulness of the medical-surgical sessions (3.69 vs 3.83; P=.30) or of the multidisciplinary team (3.63 vs 3.83; P=.18).

Both the medical-surgical sessions and the multidisciplinary teams were exclusively in-person according to 57.7% of respondents. In 11.2% of cases, they were exclusively online, whereas 31.1% of respondents reported them to be either telematic or in-person.
The surveyed professionals gave an average score of 2.97±1.2 to a question concerning whether patients undergoing complex surgical/interventional procedures received direct information from both specialties on the intervention. Nonetheless, the surgeons and cardiologists disagreed on this point with mean scores of 2.44±1.24 and 3.15±1.18, respectively (P<.001).
Finally, regarding satisfaction with the presentation of the outcomes of the respondents’ center, the average score was 2.81±1.4; this was rated 2.72±1.4 by the cardiologists and 3.07±1.4 by the surgeons (P=.04).
Joint work between the cardiovascular surgery and cardiology specialtiesIn response to a question concerning whether the professionals desire joint surgery-cardiology activities, the mean score was 3.5±1.1 (3.41±1.1 for cardiology and 3.75±1.1 for surgery; P=.01).
This concordance decreased when respondents considered the presence of surgeons or cardiologists in conferences of the other specialty (1=very insufficient, 5=excellent; mean, 2.2±0.9). For the assessment of local outcomes, the respondents gave the following scores to their referral departments: surgical, with 373 responses (mean, 3.81±0.9); and interventional cardiology, with 382 responses (mean, 4.22±0.7).
Regarding the advisability of performing interventional procedures for structural heart disease in centers without on-site cardiovascular surgery, the respondents gave a mean score of 3.02±1.4. The average concordance scores were 1.94±1.28 for surgeons and 3.38±1.26 for cardiologists (P<.001).
On this structural topic and as proposals for consideration, the respondents gave average scores of 2.77±1.2 to the collaboration between surgeons and interventional cardiologists and of 2.98±1.2 to the presence of a surgeon in the catheterization laboratory. However, greater consensus was detected in the appropriateness of centralizing some specific or more complex procedures in certain community hospitals, with an average score of 4.18±1.1. In addition, most respondents (80.5%) mentioned the existence of joint protocols or clinical pathways between surgery and cardiology and 51.2% had multidisciplinary units.
Finally, most professionals considered a poor relationship between cardiology and surgery to negatively affect patient care (4 or 5 points in 96.3% of responses; mean, 4.78±0.6).
Future and areas for improvement between specialtiesOverall, 65.2% of the respondents (382 responses) agreed that the 2 specialties should form a joint specialty with a common core and made numerous suggestions for improving them. As potential areas for improvement, the respondents highlighted the need to enhance coordination between specialties, foment teamwork by stressing the value of multidisciplinary teams, interrelate more, draft consensus documents or protocols, train together, and leave aside personal interests by being more transparent about procedural outcomes.
DISCUSSIONThe present work is the first study of the relationship between cardiology and cardiovascular surgery professionals in Spain conducted using an analysis of the current opinions of members of the SEC and SECCE.
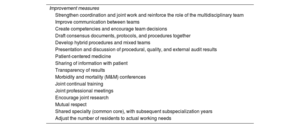
The main study findings are the following (figure 5): a) analysis of the opinions of cardiovascular surgery and cardiology professionals revealed that the respondents were generally male and attending physicians with more than a decade of experience in their field, particularly in higher-level hospitals; b) the opinions of cardiologists of their surgeon colleagues and vice versa were generally fairly good but with considerable room for improvement, and some differences in criteria were found between specialties and societies; c) the findings were similar in publicly funded centers and private centers; d) the interactions between the 2 specialties, typically occurring in medical-surgical sessions or in the multidisciplinary team, were generally satisfactory for respondents and considered very important or even necessary; and e) the room for improvement in this field is vast, and the professionals who responded to the CARDIOXCARDIO survey proposed multiple points to consider (table 2).

Proposals of the surveyed professionals
| Improvement measures |
| Strengthen coordination and joint work and reinforce the role of the multidisciplinary team |
| Improve communication between teams |
| Create competencies and encourage team decisions |
| Draft consensus documents, protocols, and procedures together |
| Develop hybrid procedures and mixed teams |
| Presentation and discussion of procedural, quality, and external audit results |
| Patient-centered medicine |
| Sharing of information with patient |
| Transparency of results |
| Morbidity and mortality (M&M) conferences |
| Joint continual training |
| Joint professional meetings |
| Encourage joint research |
| Mutual respect |
| Shared specialty (common core), with subsequent subspecialization years |
| Adjust the number of residents to actual working needs |
The current analysis of the relations between the cardiology and cardiovascular surgery specialties in Spain has provided valuable data on the perceptions and professional dynamics in this crucial field of cardiovascular medicine. The professionals invited to participate in the CARDIOXCARDIO study represent the vanguard of Spanish cardiology and cardiovascular surgery. The cooperation of all members of these 2 specialties was essential to understand the dynamics and challenges inherent to their collaboration.4,9 Despite the low response rate, the respondents’ experience and opinions provide a solid basis for the analysis of the current perspective and suggest significant improvements.
One of the key findings of this study was the generally positive view of the relationship between cardiology and cardiovascular surgery professionals. Nonetheless, this positive perception coexists with a unanimous recognition that there is considerable room for improvement. This duality indicates the complexity of the interdisciplinary collaboration in the medical field and highlights the need for an in-depth examination of the factors contributing to both efficacy and areas of opportunity. The interaction between the 2 specialties, which often takes place in medical-surgical sessions and as part of the multidisciplinary team, was identified as a positive and satisfactory factor, but frequently competitive, particularly in the field of structural interventional cardiology. This finding highlights the importance of collaborative and multidisciplinary spaces in which cardiologists and cardiovascular surgeons can share knowledge and make joint decisions for the patients’ benefit. The existence of these collaborative spaces indicates that, despite the challenges, there is a solid foundation for growth and improvement.
Taken together, the study shows wide room for improvement, and the professionals surveyed as part of the CARDIOXCARDIO survey identified various key points for optimizing relations between cardiology and cardiovascular surgery (table 2). These suggestions ranged from improvements in communication and coordination to the implementation of specific strategies for managing common challenges. The diversity of opinions and the abundance of suggestions indicate the complexity and uniqueness of each hospital environment, as well as the need for context-specific solutions. The proposed areas for improvement include the implementation of more efficient communication protocols, the endorsement of regular meetings between cardiologists and cardiovascular surgeons to discuss clinical cases and share knowledge, and the exploration of shared educational initiatives.
These suggestions would not only improve collaboration now, but also help to cultivate a new generation of cardiovascular health care professionals with a more holistic and collaborative spirit. The development of shared training pathways for both specialties and even a common core pathway could be considered, a proposal accepted by a high percentage of respondents.
In addition, the CARDIOXCARDIO results indicate that the relationship between cardiologists and surgeons is intrinsically linked to hospital structure and management. The quality of the professional relationship between these specialties is likely influenced by the internal organization, allocation of resources, and clarity of functions and other responsibilities. This connection indicates that the improvements in collaboration must address not only interpersonal aspects, but also structure and organization.
Our results also highlight the importance of feedback and continuous assessment to measure the progressive improvement in the relationship between cardiology and cardiovascular surgery.9 The establishment of key performance indicators and implementation of effective feedback mechanisms may be crucial to assess the impact of the proposed interventions and make the necessary strategic changes.8,10
LimitationsThe present work should be considered hypothesis generating due to the limitations inherent to its design and data source. Obviously, it may have a selection bias with a difficult-to-interpret direction because the study is based on data obtained from a voluntary, unpaid survey that was sent to members of 2 scientific societies. Consequently, the sample of surveyed professionals may differ from the the general population of physicians practicing in Spain, and more collaboration could be found between professionals more interested in this topic. In addition, the response rate differed between the 2 societies, which could have affected the results. Nonetheless, these results, obtained from a considerable number of professionals in the field, provide sufficiently accurate information and guidance to suggest measures for practical improvements in inter-specialty collaboration and subsequent assessment of the measures implemented.
CONCLUSIONSThe present study analyzed current relations between cardiology and cardiovascular surgery in Spain and revealed differences in scoring by specialty. The combination of positive perceptions and the suggested areas for improvement offers a strategic opportunity to implement significant changes strengthening the collaboration between these 2 disciplines. The implementation of strategies based on the suggestions of the professionals surveyed, together with a proactive focus on continual improvement, could greatly boost the quality of cardiovascular care in Spain, which would benefit both professionals and patients.
- •
The relationships among the various medical disciplines have attracted growing interest in the scientific community, particularly in the field of cardiovascular health.
- •
Cardiology and cardiovascular surgery are pivotal branches of cardiovascular medicine, with each playing complementary roles in the prevention, diagnosis, and treatment of cardiac diseases. Consequently, the existence of smooth logistical and personal relationships is becoming increasingly vital. However, collaboration between these 2 specialties is not without its challenges, controversies, and debates.
- •
The CARDIOXCARDIO study, a joint initiative of the SECCE and SEC, contacted all members of the 2 societies to invite them to complete a brief online survey evaluating multiple aspects of the working relationships between the specialties.
- •
On a scale from 1 to 5 (from worst to best), respondents assigned a mean score of 3.57±0.9 points to the relations between surgery and cardiology. Differences in criteria were detected between the specialties.
- •
The combination of perceptions and the areas for improvement offers an opportunity to significantly enhance collaboration between these 2 disciplines.
Funding was received from the Spanish Society of Cardiology for the open-access publication of this article in Revista Española de Cardiología.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCENo artificial intelligence was used in the preparation of this article.
AUTHORS’ CONTRIBUTIONSAll authors from the joint commission participated in the survey design and decision to send the surveys. In addition, they contributed to the manuscript drafting and critical revision. I.J. Núñez-Gil designed the survey interface and performed the statistical analysis and initial manuscript drafting. J. Pérez-Villacastín and J. Rodríguez-Roda, senior coauthors on this article, devised and created the joint commission, promoted the CARDIOXCARDIO initiative, and participated in its critical revision.
CONFLICTS OF INTERESTThe authors confirm the absence of conflicts of interest related to the current manuscript. This study was an initiative promoted by the Spanish Society of Cardiovascular and Endovascular Surgery (SECCE) and the Spanish Society of Cardiology (SEC).