
We have read with interest the comments by Vannini et al. regarding our scientific letter1 on ventilatory response during exercise testing in a population of patients with persistent COVID-19 symptoms. We thank the authors for their observations and comments.
In the assessment of oxygen consumption, we understand the relevance of including spirometry data with diffusing capacity for carbon monoxide (DLCO) testing, given that 43% of patients with SARS-CoV-2 sequelae have been reported to have a DLCOof less than 80% of the predicted capacity.2 We are aware of this limitation in our work and welcome the comment by Vannini et al. on future improvements to our research.
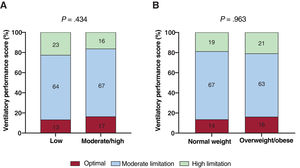
Regarding the absence of a subgroup analysis (eg, obese vs nonobese, or trained vs untrained) in explaining our previous findings,1 the figure 1 presented again shows that ventilatory inefficiency is independent of nutritional status or physical activity levels. We disagree that the protocol used in our study “may be poorly tolerated by less trained patients with symptoms of chronic fatigue”, suggesting adaptations to achieve better exercise tolerance. As previously mentioned,1 the mean exercise test time was 13.0minutes and this small difference still preserves the relationship between VO2, workload, and heart rate during cardiopulmonary exercise testing.
 and nutritional status by BMI (B) and ventilatory performance categories. The ventilatory performance criteria score is derived from the sum of the abnormal criteria, then classified as follows: no ventilatory limitation (no abnormal criteria), moderate limitation (1-2 abnormal criteria), and high limitation (more than 3 abnormal criteria). Values are expressed as No. (%). Differences were determined using the chi-square contingency test. BMI, body mass index.")
Comparison of physical activity levels (A) and nutritional status by BMI (B) and ventilatory performance categories. The ventilatory performance criteria score is derived from the sum of the abnormal criteria, then classified as follows: no ventilatory limitation (no abnormal criteria), moderate limitation (1-2 abnormal criteria), and high limitation (more than 3 abnormal criteria). Values are expressed as No. (%). Differences were determined using the chi-square contingency test. BMI, body mass index.
We agree that the pathophysiological mechanisms of COVID-19 sequelae remain uncertain, and we believe that rehabilitation, based on physical exercise, is a mainstay for the treatment of various persistent symptoms, as recently demonstrated.3 Indeed, this was the motive prompting our study.4
FUNDINGThis study was funded in part by a grant (PID2020-113098RB-I00) corresponding to the call for RD&I projects from the national programs for knowledge generation and scientific and technical strengthening of the RD&I system aimed at the challenges of society, within the framework of the National Plan for scientific and technical research and innovation 2017-2020
AUTHORS’ CONTRIBUTIONAll authors have contributed substantially to the drafting, review, and intellectual content of the manuscript.
CONFLICTS OF INTERESTNone declared.
.