
Although the increase in the worldwide prevalence of hypertension is largely caused by population aging, changes in behavior (sedentary lifestyle, obesity, increased dietary salt intake, etc.) have increased the number of individuals who develop hypertension at earlier ages.1
Thus, specific analysis of the management and degree of blood pressure (BP) control in this collective in Spain would appear to be timely. The PRESCAP 2010 (blood pressure in the Spanish population attending primary care centers) study was designed to determine the degree of BP control in a large hypertensive population managed in the primary care setting and receiving drug therapy.2 The objective of the study was to analyze the clinical profile and management of hypertensive patients by age group.
The PRESCAP 2010 study included 12 961 hypertensive individuals, of which 440 (3.4%) were younger than 45 years; 1672 (12.9%) were aged 45 to 54 years; and 10 849 were older than 54 years. As the patients aged, systolic BP increased, as did the proportion of patients with dyslipidemia, diabetes mellitus, target organ damage, and cardiovascular disease (Table 1). In contrast, patient aging was associated with decreasing diastolic BP and reductions in the proportion of smokers and of patients with a family history of cardiovascular disease.
Clinical Characteristics of the Patients According to Patient Age (<45 Years, 45-54 Years, and >54 Years)
| Variable | <45 years (n=440; 3.4%) | 45-54 years (n=1672; 12.9%) | >54 years (n=10 849; 83.7%) | P |
| Biodemographic data | ||||
| Age, years | 39.8±4.0 | 50.3±2.7 | 69.9±8.5 | .0001a |
| Men | 60.6 | 55.6 | 46.2 | .0001b |
| Systolic BP, mmHg | 131.9±14.3 | 133.6±13.5 | 136.4±14.6 | <.0001a |
| Diastolic BP, mmHg | 82.3±9.2 | 82.1±9.0 | 78.7±9.4 | <.0001a |
| Cardiovascular risk factors | ||||
| Sedentary lifestyle | 53.1 | 55.0 | 55.6 | nsb |
| Dyslipidemia | 37.8 | 52.3 | 59.8 | .0001b |
| Smoking | 37.6 | 32.9 | 13.2 | .0001b |
| FH CVD | 27.5 | 28.0 | 19.4 | .0001b |
| Diabetes mellitus | 14.0 | 21.0 | 33.1 | .0001b |
| Target organ damage | ||||
| Microalbuminuria | 11.7 | 16.2 | 19.1 | .037b |
| LVH | 3.0 | 4.6 | 8.6 | .0001b |
| Cardiovascular disease | ||||
| Ischemic heart disease | 1.8 | 4.3 | 11.3 | .0001b |
| Renal failure | 3.7 | 3.4 | 7.6 | .0001b |
| Stroke | 0.9 | 1.3 | 5.1 | .0001b |
| Heart failure | 0.9 | 0.8 | 6.0 | .0001b |
| Peripheral arterial disease | 0.9 | 1.3 | 4.4 | .0001b |
BP, blood pressure; CVD, cardiovascular disease; FH, family history; LVH, left ventricular hypertrophy; ns, not significant.
The data are expressed as % or mean±standard deviation.
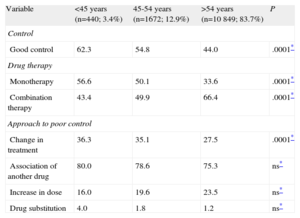
BP control worsened as the patients aged (62.3%, 54.8%, and 44.0%, respectively; P=.0001), despite the more widespread use of combination therapy (43.4%, 49.9%, and 66.4%, respectively; P=.0001) (Table 2). As patient age increased, physicians introduced fewer changes to the hypertensive therapy (36.3%, 35.1%, and 27.5%, respectively; P=.0001). The most common measure in all 3 groups was to associate another medication, followed by increasing the dose and, least frequently, changing the drug therapy, with no significant differences among the age groups (Table 2).
Degree of Blood Pressure Control, Type of Treatment, and Approach to Poor Blood Pressure Control According to Patient Age (<45 Years, 45-54 Years, and >54 Years)
| Variable | <45 years (n=440; 3.4%) | 45-54 years (n=1672; 12.9%) | >54 years (n=10 849; 83.7%) | P |
| Control | ||||
| Good control | 62.3 | 54.8 | 44.0 | .0001* |
| Drug therapy | ||||
| Monotherapy | 56.6 | 50.1 | 33.6 | .0001* |
| Combination therapy | 43.4 | 49.9 | 66.4 | .0001* |
| Approach to poor control | ||||
| Change in treatment | 36.3 | 35.1 | 27.5 | .0001* |
| Association of another drug | 80.0 | 78.6 | 75.3 | ns* |
| Increase in dose | 16.0 | 19.6 | 23.5 | ns* |
| Drug substitution | 4.0 | 1.8 | 1.2 | ns* |
ns, not significant.
The data are expressed as %.
In our study, we observed that, as the patients aged, the risk profile deteriorated, with a greater number of risk factors and greater development of target organ damage and associated cardiovascular disease. However, in the youngest patients, although other cardiovascular risk factors were frequently present, clinically evident cardiovascular disease was relatively uncommon. This result is unsurprising since atherosclerotic disease takes years to become apparent. However, because the number of associated risk factors has increased, compared with the situation in earlier decades, the clinical signs of cardiovascular disease appear at increasingly earlier ages.
Hypertension has been shown to increase the risk of cardiovascular complications in all age groups, including the youngest.3 Although adequate BP control has become more widespread in recent years, its prevalence is still far from being acceptable.4 In our study, patients aged 45 to 54 years had an appreciably higher rate of adequate BP control than those of more advanced age, and BP control was even better among those younger than 45 years. However, 40% to 45% of young hypertensive individuals in Spain do not achieve adequate BP control. Given that only treated hypertensive patients were included in the PRESCAP 2010 study, these rates may be even higher among young hypertensives in the general population. Moreover, there are probably cases of undiagnosed hypertension in this age group since these individuals usually visit their physicians less frequently and more sporadically than older persons.5
The improvement in BP control observed in recent years has been related in part to the more widespread use of combination therapy.4 In our study, somewhat less than half of the patients younger than 55 years of age were receiving combination therapy, a rate that is appreciably lower than that found among hypertensive patients aged 55 years or older. Moreover, the therapeutic regimen was modified in only slightly more than one-third of the hypertensive patients younger than 55 years with poor BP control (36% of those under the age of 45 years). All these data are probably the result, in part, of an underestimation of cardiovascular risk among young hypertensive individuals, because risk is usually assessed over the short- or medium-term, rather than over the long-term.6
In short, approximately 16% of the hypertensive patients receiving drug therapy and being managed in primary care centers in Spain are younger than 55 years of age (3.4% are younger than 45 years). Approximately 40% to 45% of the patients younger than 55 years do not achieve BP targets. In the light of all these findings, we conclude that improvement in the overall control of cardiovascular risk factors in young individual is essential and that such improvement obviously includes hypertension.
We wish to thank all the primary care physicians participating in the PRESCAP 2010 study for their collaboration in the PRESCAP 2010 study and all the members of the HTA/SEMERGEN Group (list available in supplementary material) for providing the data necessary for its performance. We also thank Almirall, S.A., for providing the infrastructure necessary for carrying out this study. Almirall, S.A., did not influence the collection or interpretation of the data.