Keywords
INTRODUCTION
Dextrocardia is generally defined as the location of the heart in right hemithorax or with the apex pointing to the right. It is very frequently associated with multiple complex congenital cardiac malformations and situs anomalies.
We report the case of a patient with multiple cardiovascular and organ abnormalities who underwent surgery for myocardial revascularization and aortic valve and ascending aorta replacement.
CASE REPORT
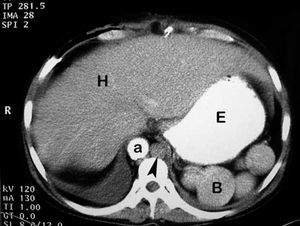
A 53-year-old man was transferred to our hospital for aortic valve replacement and myocardial revascularization. Chest radiography revealed dextrocardia. His medical history included a renal transplantation in 1994, with several rejection episodes, marginal renal function, dyslipidemia, and a diagnosis of aortic valve stenosis (orifice area of 0.6 cm2). Coronary arteriography revealed severe lesions in the left anterior descending and right coronary arteries. During the preoperative study, the patient presented a deterioration in renal function for which he required hemodialysis. Prior to surgery, he underwent a complete anatomical study of his situs anomalies. Magnetic resonance revealed dextrocardia with right-sided aortic arch and absence of the intrahepatic inferior vena cava, with azygos continuation, draining into a dilated left superior vena cava. Thoracoabdominal computed tomography revealed a centrally located liver and gallbladder, the stomach in normal position and left-sided polysplenia (Figure 1).

Figure 1. Abdominal computed tomography shows right aorta (a), enlarged azygous vein (arrow), centrally located liver (H) and stomach in normal position (E). The rounded structures (B) are multiple spleens.
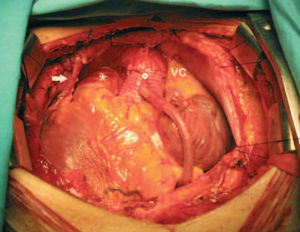
The patient underwent surgery, with the surgeon situated on the right side of the operating table. Once the pericardium had been opened, dilation of the ascending aorta was observed. Cardiopulmonary bypass was established according to the standard technique, with an aortic and a venous cannula and dual drainage in right atrium. Protection of the heart was provided by antegrade and retrograde cardioplegia. Distal anastomoses were performed, and the right mammary artery and saphenous vein were used for the left anterior descending coronary artery and right coronary artery, respectively. The patient presented a bicuspid aortic valve which was severely calcified. It was resected and replaced with a mechanical prosthesis. The ascending aorta was dilated (more than 5 cm in diameter) and its wall was thin and friable. Taking into account this dilation and the presence of a bicuspid valve, it was decided to replace the ascending aorta with a 28-mm graft (Hemashield) with which the proximal venous anastomosis was performed (Figure 2). The cardiopulmonary bypass was discontinued without incidents. The postoperative course was uneventful except for the failure of the patient to recover kidney function, a circumstance that made hemodialysis necessary. Two weeks after surgery, the patient, completely recovered, was transferred to a referral hospital to continue treatment for renal failure. At present, the possibility of retransplantation is being considered.

Figure 2. Operative field after surgery. From left to right, right internal mammary artery (arrow) anastomosed to anterior descending coronary artery, pulmonary artery (asterisk), the grafting of ascending aorta to the right coronary artery using a saphenous vein (white circle) and a markedly dilated superior vena cava (VC).
DISCUSSION
Dextrocardia should alert clinicians and surgeons to the possibility of associated cardiac malformations. Magnetic resonance imaging is the technique of choice for the evaluation of anomalous venous return1 and, in our case, it was definitive for the identification of the vascular malformations that accompany this syndrome. The presence of valve disease and the absence of intracardiac malformations were confirmed by the echocardiogram. Our patient represents a typical case of heterotaxy, or situs ambiguous, in which there is a wide range of organ and cardiac changes. Situs ambiguous associated with polysplenia is also referred to as left isomerism, in which both atria exhibit the characteristics of a left atrium, although, in this case, the appearance of the right atrium was normal. Left isomerism is the rarest of all the subcategories of dextrocardia, and interruption of the inferior vena cava is the most common vascular malformation. Its presence has technical implications for cannulation given that most of the venous return drains into right atrium via a dilated superior vena cava. There are reports concerning cardiac surgery in dextrocardia,2-7 but most of them refer to myocardial revascularization, attempted in some cases6 and performed without cardiopulmonary bypass in others,4,5 and in patients with situs inversus. Our case is the first involving situs ambiguous associated with polysplenia in which 3 cardiac procedures were performed (coronary arteries, valve, and aorta). The decision to replace ascending aorta was made upon the observation of a dilated aorta in the context of bicuspid aortic valve stenosis, a condition recently reported in a patient with dextrocardia.8 It is highly probable that the renal failure presented by the patient accelerated the calcification of the aortic valve and the progression of coronary atheromatosis.
Received December 9, 2004.
Accepted for publication January 27, 2005.
Correspondence: Dr. A. Arís.
Servicio de Cirugía Cardíaca. Hospital de la Santa Creu i de Sant Pau.
San Antonio M. Claret, 167. 08007 Barcelona. España.
E-mail: aaris@santpau.es