Evidence from clinical trials and ‘real-world’ studies has demonstrated that direct oral anticoagulants (DOAC) are as safe or safer than vitamin K antagonists (VKA) and at least as effective at preventing embolic events; DOACs are therefore now recommended as the first-line anticoagulation therapy in clinical guidelines.1 Nevertheless, use of DOACs in Spain is limited and lower than that of comparable countries.2 While this situation may be related to restrictions imposed by the Spanish health care system,2 there is also evidence that VKA prescription is influenced by physicians’ perceptions and attitudes.3 Our aim in the present study was to analyze Spanish cardiologists’ perceptions of the quality of anticoagulation with VKAs and to compare this perception with real-world evidence.
The cardiology services of all hospitals within the Spanish national health system were invited to participate in the study. In total, 171 centers agreed, and the heads of service at each hospital selected members of their teams to participate. A total of 588 cardiologists were interviewed by an external company between April and May 2018. The study participants were not forewarned of the study objectives. Each participant was asked to access his or her center's records and retrieve the medical history of a patient with nonvalvular atrial fibrillation (NVAF) who had attended the clinic that same day; the cardiologist was asked to assess the patient's international normalized ratio (INR) and time in therapeutic range (TTR). Participants were also asked to recall the last 4 NVAF patients treated with VKAs at their clinics and to state whether these 4 patients were correctly anticoagulated (TTR> 65% in the previous 6 months). Interviews were conducted at the end of clinics, and cardiologists gave informed consent to participate. Data calculated as means were compared by the Student t test and proportions were compared by the chi-square test. Differences were considered statistically significant at P<.05.
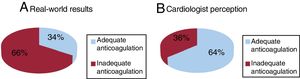
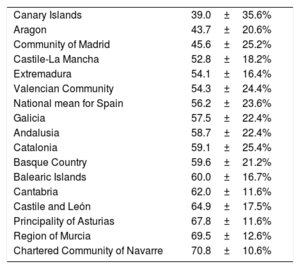
Interviews were conducted with 588 cardiologists from 171 cardiology services distributed across all Spanish autonomous communities. Of the cardiologists interviewed, 37% were women and 49% were younger than 40 years. Overall, 33% of the cardiologists were unable to directly access the patient's medical history and INR/TTR data, either on paper or on a computer database; moreover, access to this information varied considerably between autonomous communities (P <.001). The time needed to assess the INR and TTR was 1.16±1.40minutes. Mean TTR was 56.2±23.6%, ranging from 39% in the Canary Islands to 70.8% in the Chartered Community of Navarre (P <.001; table 1). Only 36% of patients had a TTR> 65%, with the remaining 64% of patients inadequately anticoagulated (figure 1A). In contrast, according to the cardiologists’ recollections of the 4 most recent VKA-treated NVAF patients in their clinics (N=756), anticoagulation was inadequate (TTR <65%) in only 36% of patients (272 of 756) (figure 1B). This result was similar for all autonomous communities. Neither real-world data nor cardiologist perception differed according to cardiologist sex or age range. Overall, male cardiologists believed 66.3% of their patients to be adequately anticoagulated, vs the true value of 35.4%, while the corresponding figures for female cardiologists were 63.1% and 34.8%. Cardiologists younger than 40 years believed anticoagulation to be adequate in 67.3% of patients overall, vs a real value of 35.2%, and the corresponding figures for cardiologists aged 40-55 years and>55 years were 66.3% versus 34.4% and 62.5% vs 37.8%, respectively.
Time in therapeutic range by autonomous community and nationally
| Canary Islands | 39.0±35.6% |
| Aragon | 43.7±20.6% |
| Community of Madrid | 45.6±25.2% |
| Castile-La Mancha | 52.8±18.2% |
| Extremadura | 54.1±16.4% |
| Valencian Community | 54.3±24.4% |
| National mean for Spain | 56.2±23.6% |
| Galicia | 57.5±22.4% |
| Andalusia | 58.7±22.4% |
| Catalonia | 59.1±25.4% |
| Basque Country | 59.6±21.2% |
| Balearic Islands | 60.0±16.7% |
| Cantabria | 62.0±11.6% |
| Castile and León | 64.9±17.5% |
| Principality of Asturias | 67.8±11.6% |
| Region of Murcia | 69.5±12.6% |
| Chartered Community of Navarre | 70.8±10.6% |
 according to (A) real-world data and (B) surveyed cardiologists’ perceptions.")
Our study reveals poor anticoagulation with VKAs in NVAF patients treated in Spanish cardiology clinics; moreover, the detected quality of anticoagulation is worse than that reported in recent Spanish studies.4,5 In those earlier studies, TTR was below 65% in 40% to 50% of patients, whereas in our study the value was 64%. Furthermore, our study shows that almost a third of cardiologists could not access INR and TTR data for patients treated at their centers. The discouraging real-world data contrast with the optimistic perceptions among the surveyed cardiologists, who believed that good control was achieved in 64% of patients, almost double the true rate. Although this study has limitations, including the lack of randomization of the participating cardiologists, there is clearly a notable discrepancy between the real and cardiologist-perceived quality of anticoagulation achieved with VKAs. Together with other likely causes noted above,2 this discrepancy is likely to influence the underuse of DOACs in Spain.
CONFLICTS OF INTERESTThis study was carried out by the Spanish Society of Cardiology Research Agency with unconditional financial support from Daiichi-Sankyo. All the authors have received payments from the Spanish Society of Cardiology for their participation in the study scientific committee.