



Although venoarterial extracorporeal membrane oxygenation (VA-ECMO) provides effective cardiocirculatory support in patients with fulminant myocarditis, the most effective timing of venting is uncertain. We aimed to investigate the benefit of early venting among patients who underwent VA-ECMO for fulminant myocarditis.
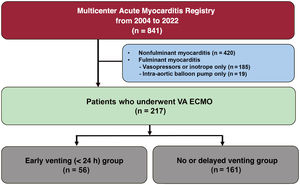
MethodsAmong 841 patients with acute myocarditis from 7 hospitals in the Republic of Korea, 217 patients with fulminant myocarditis who underwent VA-ECMO were included in this analysis. The patients were categorized into 2 groups: an early unloading group that underwent venting within 24hours of ECMO insertion, and the no or delayed unloading group. The primary outcome was a composite of death, cardiac replacement, or cardiovascular rehospitalization.
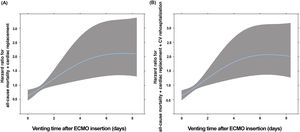
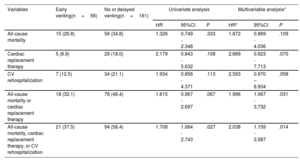
ResultsAmong 217 patients, 56 underwent early venting, 54 underwent delayed venting, and 107 did not undergo venting. On spline curves in 110 patients who underwent venting, rapid deterioration was observed as the timing of venting was delayed. The incidence of the primary outcome was lower in the early venting group than in the no or delayed unloading group (37.5% vs 58.4%; HR, 0.491; 95%CI, 0.279-0.863; P=.014). Among patients not experiencing the primary outcome within 6 months, clinical outcomes were similar after 6 months (P=.375).
ConclusionsEarly left heart unloading within 24hours of ECMO insertion is associated with a lower risk of a composite of death, cardiac replacement therapy, and cardiovascular rehospitalization in patients with fulminant myocarditis undergoing VA-ECMO. Registered at ClinicalTrials.gov (NCT05933902).
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm