To the Editor,
A 68 year old man with symptomatic aortic stenosis was referred to our institution for aortic valve replacement. Coronary angiography had been performed to exclude significant coronary disease.
The coronary angiogram identified an abnormally high ostium of the right coronary artery (RCA) which necessitated difficult nonselective catheterization. A multidetector computed cardiac tomography (MDCT) was performed to identify accurately the anomalous coronary origin. A high origin for coronary arteries has been defined as having ostia originating between 5 and 10 mm above the Sinotubular Junction (SJ). In our case, the MDCT showed the RCA was located 20 mm (mean distance) above the SJ and originated at an acute 30o angle (Figure 1) and movie. The height of the origin of the vessel was important in relation to the angle of take-off from the aortic wall since it has been postulated that a high ostium results in decreased coronary perfusion.1 The anomalous origin of this artery was a sacular cavity as described in other reports. In the literature this part of the coronary artery was thinner, similar in composition to the aortic wall. The special configuration of the coronary ostium and the elasticity of the origin of the RCA maintained patency of the artery during the cardiac cycle.

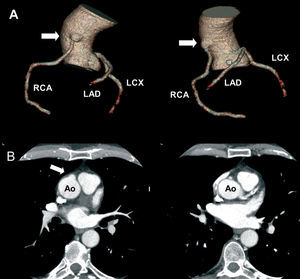
Figure 1. A: volume rendering with tree representation of coronary arteries. RCA indicates right coronary artery, LCX, left coronary circumflex, LAD, left anterior descending. Ectopic origin of RCA (arrow). B: left: MDCT axial image at origin of RCA (arrow) showed the sacular cavity at ostial level; right: MDCT axial image at the normal origin of left coronary artery at left coronary sinus.
The orifice was not collapsed as a slit-like ostium and there was no diastolic entrapment from the initial investment in aortic adventitia. Our case had a benign outcome, thanks to the important information derived from MDCT which allowed the cardiac surgeon to avoid accidentally cross-clamping or transecting this vessel during surgery.