To the Editor,
A prolonged corrected QT interval (cQT) during coronary ischemia is a well known sign that has even been incorporated into the parameters tested for the assessment of ischemic risk in acute coronary syndrome (ACS).1 There is also a correlation between a long QT and helicoidal ventricular tachycardia, or torsade de pointes (TdP), that has been described in this context.2 Here, we present a case of ACS with a very prolonged QT interval with giant negative T-waves and a later development of TdP.
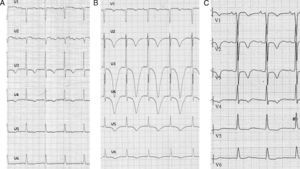
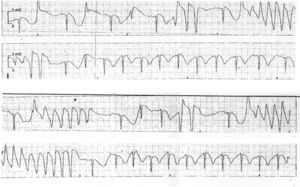
A 79-year-old woman sought emergency treatment for diffuse pain in the anterior thorax and dyspnea with 2 days evolution. She had a background of type-2 diabetes mellitus, systemic arterial hypertension, and rheumatoid arthritis. She was under treatment with metformin, vildagliptin, losartan, and indometacin. Upon admission to the hospital, the patient was dyspneic with a blood pressure of 219/96mmHg, an O2 saturation of 86%, and a regular pulse at 98 bpm, with notable bilateral basal crepitation. The abdomen was without abnormalities, with intact peripheral pulse. The initial electrocardiogram (ECG) (Figure 1A) demonstrates a sinus rhythm of 94bpm, PR of 125ms, QRS of 9ms, without a significant decrease in ST, asymmetrical negative T-waves at V3 and V5, and a cQT of 510ms. Laboratory analyses indicated normocytic hypochromic anemia, creatinine at 1.4mg/dl, sodium at 138mEq/l, potassium at 4.5mEq/l, and magnesium at 1.8mg/dl. The troponin T test was positive for myocardial injury. An echocardiogram indicated that the left ventricle had septal hypertrophy, septoapical hypokinesia and anteroapical akinesia, with an ejection fraction of 39%. The diagnosis was made of non-ST elevation left heart failure in the context of ACS, hypertension, and normocytic anemia. The patient was treated using double antiplatelet, anticoagulant, and vasodilator drugs. After 24h, the patient was stable, with blood pressure at 140/85mmHg and the control ECG (Figure 1B) demonstrated giant negative T-waves from V2 to V5 with a cQT of 745ms. We monitored the patient using ECG, revealing bouts of type TdP polymorphic ventricular tachycardia (Figure 2), which ceased upon intravenous administration of 2g magnesium sulphate. Serial measurements of markers for myocardial damage were congruent with a myocardial infarction, excluding other possible causes of the prolonged cQT.

Figure 1. A, test results upon admission: RR, 640ms; corrected QT interval, 510ms. B, test results after 24h: RR, 780ms; corrected QT interval, 745ms. C, test results after 13 days: RR, 760ms; corrected QT interval: 504ms. (Corrected QT intervals derived using Bazett's formula.)

Figure 2. Torsade de pointes (electrocardiogram monitoring following Figure 1 B).
A cardiac catheter test demonstrated a calcified lesion along 10% of the common arterial trunk and a lesion along 70% of the anterior descending artery. We treated the patient by implanting a stent, and later evolution was favorable. A control echocardiogram indicated that the patient did not suffer contractile deficit, and systolic function was normal. In the ECG taken 13 days later (Figure 1C), the negative T-waves continued between V1 and V5, and the cQT remained at 504ms. The QT interval normalized after 6 weeks.
The relationship between myocardial ischemia and a reversible prolongation of the QT interval has been shown during controlled coronary occlusion in angioplasty procedures, and it has been documented that prolongation of the cQT is the most concordantly altered electrocardiographic variable during the early phase of transmural ischemia.3 The incidence of helicoidal ventricular tachycardia in myocardial infarctions is close to 2%,2, 4 and is most closely associated with occasional extremely prolonged cQT. These cases have been discussed under the term of acquired long QT syndrome associated with infarction.4 TdP ventricular tachycardia associated with prolonged cQT infarction tend to be preceded by the (pause-dependent) short-long-short cycle phenomenon, and its appearance is greatest in the days directly following an infarction.4
As research continues to delve into the exact mechanisms by which the QT interval is prolonged in ACS, there is ever more information regarding its etiology and implications. The underlying structural mechanisms of prolonged QT intervals are related to the increase in electric heterogeneity due to ischemia-induced changes in the ion permeability of the sodium/potassium pump and an increase in the duration of myocytic membrane potentials in the different levels of the myocardium, the middle myocardial layer in particular, with consequent uncoupling and dispersion of the repolarization.4, 5 Other studies have proposed the role of genetic causes, such as in other long QT syndromes. A mutation has been detected on the SCN5A gene, associated with altered sodium channels in one patient with an arrhythmic storm during an acute infarction. The polymorphisms known to cause the long QT phenotype have been observed between days 2 and 11 following an infarction, which provides the foundation for a genetic predisposition to prolonged QT intervals and the appearance of TdP.6
.
Corresponding author: mvilaseca@salutms.cat