
We present a family with a history of atrial arrhythmias requiring a pacemaker (PM) due to sick sinus syndrome (SSS) and paralysis of the atrium. Genetic study revealed the presence of the SCN5Ap.Arg219His variant already associated with familial paralysis of the atrium (FPA), conduction disorders, and dilated cardiomyopathy. To the best of our knowledge, this is the first report of FPA in a Spanish family.
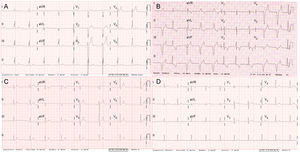
The index case (III.3) was a 30-year-old man with no relevant medical history who was admitted for dizziness; on arrival at hospital, the electrocardiogram (ECG) revealed absence of atrial activity and idioventricular rhythm (Figure 1A). The echocardiogram showed a severely dilated left atrium (60mL/m2), while the other chambers were of normal size. The left ventricular ejection fraction (LVEF) in the magnetic resonance imaging study was 48% and there was no late enhancement. A dual-chamber PM was implanted. The patient improved without any complications and left ventricular ejection fraction completely recovered after 9 months of ramipril therapy.
. B, electrocardiogram of case II.3 (age 62 years). C, electrocardiogram of case III.8 (age 32 years). D, electrocardiogram of the asymptomatic carrier II.8 (age 58 years).")
Electrocardiograms of several carriers of the p.Arg219His mutation in SCN5A. A, electrocardiogram of the index case III.3 (at age 30 years). B, electrocardiogram of case II.3 (age 62 years). C, electrocardiogram of case III.8 (age 32 years). D, electrocardiogram of the asymptomatic carrier II.8 (age 58 years).
The patient's father (II.3) required a PM at the age of 31 years, also for paralysis of the atrium. In the most recent ECG, sinus rhythm alternated with VVI pacing (Figure 1B). A paternal aunt (II.2) required a PM aged 62 years and his son (III.1) had a stroke aged 38 years and required a PM for SSS. A first cousin (III.3) had atrial fibrillation and atrial flutter from the age of 29 years, with several cardioversions, and ablation of the cavotricuspid isthmus, after which he was in sinus rhythm with propafenone (Figure 1C). The most recent echocardiogram showed dilatation of 2 chambers (left atrium 45.5mL/m2) with normal biventricular function.
The familial cluster of SSS requiring a PM at a young age led to suspicion of the presence of a genetic condition of autosomal dominant transmission (Figure 2). A genetic ultradeep sequencing study of 132 genes associated or potentially associated with arrhythmias and cardiomyopathies was ordered for the index case. Two heterozygous mutations not present in controls were found in 2 genes previously associated with conduction disorders: NC_000003.11:g.38655281C>T in SCN5A and NC_000015.9:g.73615231C>T in HCN4, as well as the polymorphism NC_000021.8:g.35821680C>T in KCNE1 associated with acquired prolonged QT interval.
/HCN4p.Arg1068His (variant of unknown significance).")
Family tree and study of SCN5Ap.Arg219His and HCN4p.Arg1068His mutations. The boxes and circles represent males and females, respectively. The shaded symbols indicate affected individuals. A dot inside the symbol indicates an individual not affected. The letter N inside the symbol indicates an individual who is not a carrier and is not affected. The symbols + and – represent carriers and noncarriers, respectively, of the mutations in individuals with available genetic studies. A diagonal line through the symbol indicates an individual who has died. The age of the individual at the time of the event is shown in parenthesis. The actual age or age on death is shown at the top right of the symbol. AF, atrial fibrillation; CE, clinical examination; ECG, electrocardiogram; LV, left ventricular; PM, pacemaker; SSS, sick sinus syndrome; TTE, transthoracic echocardiography; y, years. SCN5Ap.Arg219His (pathogenic)/HCN4p.Arg1068His (variant of unknown significance).
The SCN5Ap.Arg219His mutation has been reported in 2 families in Switzerland and Japan.1,2 Clinically, in addition to SSS, supraventricular and ventricular tachyarrhythmias may be present and a PM may need to be implanted at a young age, particularly in men. In one of the families, cosegregation of the mutation with dilated cardiomyopathy was demonstrated.1,2
In contrast, the HCN4p.Arg1068His variant had not been described previously. The HCN4 gene encodes subunit 4 of the HCN channels, which carry the native If current. These channels participate in the generation and modulation of the cardiac activity of the PM. Certain mutations in HCN4 are associated with a faster channel deactivation time, leading to loss of function and bradycardia.3 The in silico study of HCN4p.Arg1068His, was inconclusive.
A clinical-genetic study was offered to the families prior to signing the informed consent. Echocardiogram and ECG studies were conducted in 10 family members and genetic studies (when indicated) were performed in 7.
The SCN5Ap.Arg219His mutation was present in all affected persons in the paternal family. The phenotype was very similar to that described earlier, although in the literature, SSS was reported in unrelated patients.1,2 This is therefore the first time that cosegregation of SCN5Ap.Arg219His with familial paralysis of the atrium1,2 has been reported (Figure 2). In addition, 2 women aged 58 years and 34 years (II.8 and III.7, respectively) were identified as asymptomatic carriers. This finding fits with the later clinical presentation in women (Figure 1D).
The HCN4p.Arg1068His mutation and the KCNE1p.Asp85Asn polymorphism were transmitted by the mother, whose clinical study was normal. It was not possible to study the other members of the mother's family. Given that lack of cosegregation with SSS, HCN4p.Arg1068His is considered a variant of unknown significance that does not explain FPA.
Sick sinus syndrome is defined as abnormal formation and propagation of the electric impulse in the sinus node. It is characterized by sinus bradycardia, sinoatrial block, sinus arrest, chronotropic incompetence, and/or atrial tachyarrhythmias (essentially atrial fibrillation). It is a common disorder in elderly individuals but rarely seen in young people. A permanent PM needs to be implanted in approximately 50% of affected individuals.4 According to data from the Spanish Pacemaker Registry,5 SSS and atrial fibrillation/atrial flutter with bradycardia account for approximately 36% of PM implantations. There does not appear to be any predominance of one sex or the other (ratio of men to women, 0.98) although atrial fibrillation/atrial flutter with bradycardia occurs predominantly in men (ratio, 1.7).5
We consider the SCN5Ap.Arg219His mutation the cause of the familial condition as it shows cosegregation with the disease and has been described previously. The HCN4p.Arg1068His mutation is a variant of unknown significance that could act as a disease modifier, although it is not the cause. These findings would enable genetic counselling to be provided to individual carriers (Figure 2). In the case of asymptomatic patients, follow-up with electrocardiogram, Holter, and echocardiographic studies (given the association with dilated cardiomyopathy) were planned, and, depending on the symptoms, exercise testing was considered to detect chronotropic incompetence. The familial study, in this case, was essential to clarify which of the documented genetic variants was the cause of the familial paralysis of the atrium.
FUNDINGThis study was partly funded by the Instituto de Salud Carlos III (grants PI14/0967, RD12/0042/0049, and RD12/0042/0066).