Keywords
INTRODUCTION
The introduction of highly sensitive and specific biomarkers and the use of highly accurate imaging techniques in patients with acute myocardial infarction (AMI)1,2 have not eclipsed the analysis of the initial electrocardiogram (ECG), either in the indication for acute reperfusion therapy when ST segment elevation is detected (STEMI),3-5 or in the identification of electrocardiographic variables of prognostic value.6-9
There is a certain body of evidence showing that, under normal conditions, the ECG in women reveals a shorter QRS duration, a shorter PR interval and lower R, S, and T-wave voltages in precordial leads.10,11 Recently,2 in agreement with the differences observed between healthy men and women,12 the proposal has been made to employ different electrocardiographic diagnostic criteria for ischemia, and, specifically, for ST segment elevation, the application of normal limits based on sex has been proposed.2
Despite the above mentioned body of evidence, in the context of STEMI or other ischemic conditions, few publications have dealt with the possible differences between the ECG findings in men and women.13-15 From these observations, it has been deduced that ST segment deviation is of lesser magnitude in women, and it has even been postulated that the less frequent utilization of reperfusion therapies in these patients could be a consequence of the less marked echocardiographic expression of ST segment deviation in the initial ECG.15 The magnitude of ST segment elevation has also been reported to be a determining factor in the introduction of revascularization therapies and is, in turn, a prognostic marker.6,9
On the basis of the aforementioned findings, we propose to determine the possible sex-related differences in the initial ECG of patients with STEMI who are admitted early, especially in terms of the magnitude of ST segment elevation, and whether sex is an independent variable associated with a marked elevation of the ST segment.
METHODS
Between January 1998 and July 2005, all the patients admitted into 2 coronary care units of 2 tertiary hospitals within the first 24 hours after having an AMI were included in a prospective, observational, longitudinal study. The diagnosis of AMI was established on the basis of the presence of at least 2 of the following criteria: typical chest pain lasting more than 30 minutes; electrocardiographic changes indicative of ischemia or necrosis; and an increase in creatine kinase-MB isoenzyme (CK-MB) greater than or equal to twice the normal value. For the purposes of this study, we included only those patients who had no history of infarction and who, in addition, met the following criteria: evidence of ST segment elevation; admission within the first 3 hours of the onset of the symptoms; and the availability of an initial ECG tracing of sufficient quality to enable the performance of the appropriate measurements. ST segment elevation acute myocardial infarction was defined by the presence of a presumably new elevation of the ST segment in at least 2 precordial leads with a minimum value greater than 0.2 mm (0.2 mV) in the case of V1, V2, or V3 and greater than 0.1 mm (0.1 mV) in the case of the lateral or limb leads (aVL and I), inferior leads (II, III, and aVF) or V4-V6.1 The Q wave was considered to be pathological in the initial ECG when it met the following criteria: any Q wave in leads V1-V3 or a Q wave greater than 30 milliseconds in leads I, II, aVL, aVF, V4, V5, or V6.1 For an accurate measurement of ST elevation, all the patients with bundle branch block, supraventricular or ventricular tachycardia, including atrial fibrillation, high grade atrioventricular block with wide QRS escape rhythm and/or any primary abnormality associated with repolarization that could modify the expression of ischemia or injury (for example, hyperkalemia) were excluded. All the measurements were performed by 2 researchers (JGT and AMM), who were blinded to the sex of the patient to whom each tracing corresponded. The initial ECG variables analyzed were: cardiac rhythm, heart rate, frontal plane axis and QRS duration, pathological Q waves, number of leads with ST segment elevation or depression, total elevation of the ST segment and total depression of the ST segment (in both cases, the summation [SST] in millimeters in all the leads affected). ST elevation or depression was measured 0.06 seconds after the J point in the affected leads. The infarction was considered to be anterior (leads V1-V4), inferior (II, III, and aVF), regardless of whether or not right precordial leads V3R-V4R were affected, or lateral (leads I-aVL and/or V5-V6). When the localization was anterior or inferior, the concomitant ST elevation in lateral or inferior leads was included in the measurement of the total ST elevation. Intraobserver variability in the measurement of the total ST segment elevation was evaluated on the basis of the concordance in 110 repeated measurements using a Bland-Altman plot. The difference in the mean plus or minus the standard deviation was -0.7 (1.1) mm, with only 5% of the data falling outside the mean plus or minus the standard deviation. For the purpose of this study, using frequency distribution, the total ST elevation was considered according to terciles. Marked ST elevation was empirically defined as that included in the top tercile (>11 mm). The history and characteristics of the patient (age, height, and weight), the time elapsed between the onset of the symptoms and admission, heart rate, arterial blood pressure, and Killip class were all collected prospectively at admission, and the treatments, including reperfusion, procedures, and complications were also recorded. All the patients were followed from the time of admission until their death or day 31 after the diagnosis of the disease. The statistical analysis (SPSS®, version 15) was used to compare the outcomes in the 2 sexes. The relationship between dichotomous variables was established using contingency tables and c2 analysis. The quantitative variables were compared by means of ANOVA with comparison of the means using Student' t test. A P value less than .05 was considered significance. The intervals between the onset of symptoms and admission were compared by means of the Mann-Whitney U test. Age, sex, body mass index (BMI) (as a continuous and dichotomous variable, BMI ≥30), history of diabetes, hypertension, active smoking, angina, heart failure and stroke, delay after the onset of symptoms (in minutes as a continuous variable), heart rate, and arterial blood pressure at admission, and anterior localization of the infarction were included in the stepwise multivariate logistic regression analysis to determine their independent association with the presence of a marked total ST segment elevation (>11 mm). To verify the adequacy of the model, Hosmer-Lemeshow goodness-of-fit was applied.
RESULTS
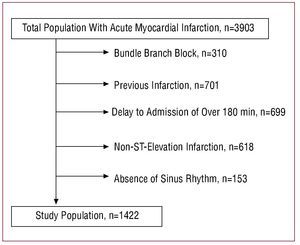
During the period of study of the 3903 patients admitted with a diagnosis of STEMI, 1422 cases were selected for the present study (Figure 1). The characteristics of the patients in our study are shown in Table 1. The 31-day mortality among women was 17.8%, versus 5.3% in men (P<.001). With respect to the peculiarities of the initial ECG, women had higher heart rates, with a difference that was nearly statistically significant, and pathological Q waves were detected more frequently. Differences in the QRS duration were not observed, although the axis was more horizontal in women. There were no differences with respect to the location of the infarction. There were no sex-related differences in the number of leads showing ST segment elevation or depression or in the total magnitude of ST segment depression. However, female sex was associated with a lesser total ST segment elevation (10 [6.6] mm vs 11.1 [7.9] mm; P<.004) and less frequently with a marked increase in the total ST segment elevation (26.4% vs 35.5%; P<.005). When anterior, inferior and lateral locations were considered separately, there was a lesser, although not significantly so, total ST segment elevation in women (Table 2).

Figure 1. Selection of the patients included in the study.


In comparison with the patients having a lesser degree of ST segment elevation, those with a marked elevation (>11 mm) were younger, with a lower proportion of women, were more frequently smokers and histories of diabetes, hypertension and angina were less common. At hospital admission, the location of the infarction was anterior in a higher proportion of the patients with marked ST segment elevation, who underwent reperfusion therapy more frequently, whereas, they presented more frequently with signs of heart failure. The marked ST elevation also corresponded with a higher maximum CK-MB value, lower left ventricular ejection fraction, a higher incidence of heart failure and a higher 31-day mortality rate (8.8% vs 6%; P<.04) (Table 3).

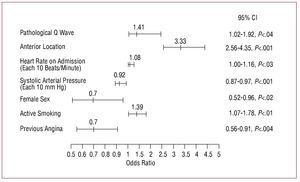
In logistic regression analysis, among other variables, female sex (odds ratio [OR] = 0.70; 95% confidence interval [CI], 0.52-0.96; P<.02) and a history of angina (OR=0.70; 95% CI, 0.56-0.91; P<.001) were inversely associated with and independent of the presence of a marked total ST segment elevation in the initial ECG (Figure 2).

Figure 2. Variables independently associated with a marked ST segment elevation in multivariate logistic regression analysis. CI indicates confidence interval.
DISCUSSION
To the best of our knowledge, this is the first study with a relatively large population of patients with STEMI and early admission in which it has been established that, independently of other peculiarities, the women had a lower magnitude of total ST segment elevation, and marked ST elevation (>11 mm) was less frequent. Among other variables, female sex was inversely and independently associated with a marked initial ST segment elevation.
Although statistical significance was not reached, the higher heart rate in women coincides with the observations reported in other studies,16-19 probably as a consequence of the high proportion of heart failure at admission. With respect to the presence of Q waves in the initial ECG, despite the exclusion of the patients with a history of infarction and the consideration of a relatively short delay until admission, this finding was observed in 19% of the women and in 15.6% of the men. These percentages were lower than the 33% reported by Andrews et al,20 in a study in which, in addition to the fact that the two sexes did not differ in terms of the incidence of Q waves, the limit considered for the delay was one hour longer than ours. In this respect, Wong et al,21 in a population in which 15% of the patients had a history of infarction, and an interval between the onset of symptoms of AMI and admission of up to six hours, found Q waves in 67% of the cases, a percentage that was markedly reduced when the analysis was limited to the patients who had been admitted within the first 2 hours. In any case, the increased presence of Q waves among the women in our study may be a consequence of the greater delay in admission,21-23 their advanced age-a factor associated with the difficulty in accurately establishing the moment of the onset of symptoms- and the higher proportion of patients with diabetes mellitus, a condition associated with silent ischemia24,25 and unrecognized previous infarction.26
Regarding the major objective of the present study, the degree or magnitude of ST segment elevation, Raitt et al15 documented a more marked ST segment elevation among women in the case of STEMI located anteriorly, although the differences were not statistically significant. In this respect, Dellborg et al13 observed a low magnitude in the ST segment elevation in women both in the presence of spontaneous ischemia and during angioplasty. Finally, Pelter et al14 documented the greater, although not significantly so, ST elevation in men during the performance of angioplasty in anterior descending and circumflex coronary arteries, although it was not observed when right coronary artery was involved. This study included a small number of patients, 20 women and 25 men, although the results are of interest because a single vessel was involved in every case and the difference in age between the 2 sexes was 3 years, much less than the 8 years in our case.
The fact that, in our study, the marked ST segment elevation is associated with a greater extension of necrosis, evidenced by higher CK-MB values, lower ejection fraction and a higher proportion of heart failure and mortality, is in accordance with the evidence of a relationship between the degree of ST segment elevation and the final size of the infarction, both in the anterior and inferior location.27-29
The inverse and independent association between the female sex and marked ST elevation may be a consequence of different circumstances. First, anatomical particularities can play an important role. For example, the lower ECG voltages in women, especially in the precordial leads,10,12 may be a consequence of the presence of less myocardial mass10 and/or the more abundant mammary fat pad, a tissue with a high electrical impedance,30 which may attenuate the recorded voltage. Obesity, more common in the female sex, is associated with a shift to the left of the QRS axis, which is more horizontal,30 factors that can contribute to reducing the ECG expression in the case of ST segment elevation. Another possible explanation for the difference in the expression of the wave produced by epicardial injury is previous angina.31,32 Although in our case, we found no differences between the 2 sexes in terms of the frequency of previous angina, it was not taken into consideration whether or not the angina had been recent. Thus, since recent onset angina is a better marker of a preconditioning stimulus,33,34 we can not rule out the possibility that this be a sex-related peculiarity. Active smoking is also associated with the presence of marked ST elevation, a finding that could depend on the younger age and, thus, the lower incidence of comorbidity in smokers, especially obesity, which, as was mentioned above, can contribute to a reduced ECG expression. Moreover, regardless of the underlying mechanisms of the so-called "smoker's paradox,"35 this habit is associated with coronary spasm,36 which is frequently characterized by a marked ST elevation.37,38 The association of an anterior location with marked ST elevation appears to be clearly related to the fact that this is accompanied by a greater extension of the infarction and by the corresponding ECG expression.39
With respect to other findings associated with marked ST elevation, increased heart rate and lower arterial blood pressure on admission may be attributed to the fact that both usually reflect a greater extension of the infarction and more frequent heart failure on admission.19,40,41 We find it more difficult to explain why Q waves in the initial ECG are associated with a marked ST elevation, unless we consider them to be the expression of a lower incidence of spontaneous reperfusion42 and the resulting partial resolution of ST elevation prior to admission.
Study Limitations
The present study can not avoid the limitations derived from the methodology. On the one hand, obesity, which attenuates electrical voltages, can be accompanied by myocardial hypertrophy, which, in turn, is related to ECG expressivity. Thus, electrocardiographic evaluation of the degree of hypertrophy could have contributed to establishing more accurately the relationship between the size of the heart and the voltages. Moreover, previous angina was not considered in terms of how long ago it had occurred, a circumstance that may have influenced the multivariate model. Likewise, it was not established whether or not the differences in ST elevation could be attributed to the territory and level of the coronary occlusion that caused the infarction. Thus, there is no evidence as to whether or not these are sex-related peculiarities. Finally, the study did not consider the degree of ST elevation in each of the affected leads separately, and it was limited to the patients admitted to the respective coronary care units. Thus, it would have been more interesting to include all the patients who presented in the emergency service with suspected AMI and minimal ST elevation.
CONCLUSIONS
In the case of patients admitted to the coronary care unit with STEMI within the first three hours of onset, women, as compared to men, have a less marked ST segment elevation and a lower incidence of marked ST elevation. Despite the limitations of the present study, our results indicate that the lower ECG expressivity in women makes it necessary to pay special attention to them in order to avoid establishing an incorrect diagnosis of absence of ST elevation, which would lead to a delay in reperfusion therapy or the decision that it is not indicated. Our findings encourage the performance of studies that include all the patients who present with suspected AMI and a slight ST segment elevation in order to evaluate to what extent the reduced electrocardiographic expression in women may lead to an underestimation of the diagnosis of STEMI.
ABBREVIATIONS
AMI: acute myocardial infarction
CK-MB: creatine kinase-MB isoenzyme
ECG: electrocardiogram
STEMI: ST-elevation myocardial infarction
Correspondence: Dr. J. Galcerá Tomás.
Unidad Coronaria. Hospital Universitario Virgen de la Arrixaca.
Ctra. de Cartagena, s/n 30120 El Palmar. Murcia. España.
E-mail: jose.galcera@carm.es
Received March 14, 2008.
Accepted for publication September 5, 2008.