
Several national1 and international2 studies have examined differences by gender in health care delay in patients with acute myocardial infarction (AMI). These studies have generally shown that delay times are longer in women than in men. Nevertheless, the results have been highly disparate due to differences in methodology and heterogeneity in the populations studied. In particular, different criteria were used to define AMI in studies carried out before 2001.3
We performed a prospective study to analyze delay times in the Cardiology Critical Care Unit of the Marqués de Valdecilla University Hospital between 2007 and 2009. We used a paired cohort design based on the age of the women included. A total of 203 patients were recruited consecutively into the study. Individuals diagnosed with the new diagnostic criteria for AMI3 were eligible for inclusion in the study with no restriction on age. Patients who had a cardiac arrest before admission, those who did not speak Spanish or who had cognitive disorders were excluded from the study. Thirty-six patients were excluded due to the lack of reliable data. Data were obtained from clinical records and a standardized questionnaire completed by cardiology critical care unit nurses during a face-to-face interview with the patient performed after admission and within 48h of the AMI. Contact delay time was defined as the time (in minutes) from symptom onset until the first medical contact. Transfer delay time was the time from the first request for assistance to arrival at the hospital, and total prehospital delay (TPD) was the time (in minutes) from symptom onset to arrival at the emergency department.
We used SPSS 15.0 for the statistical analysis. All delay times were expressed as medians [interquartile range]. To test for differences by gender we used the Wilcoxon and Mann-Whitney tests and logistic regression analysis using the ‘enter’ method.
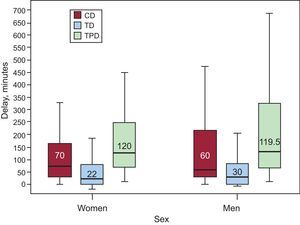
A total of 370 patients were included in the study, of which 188 were women. Mean age was 67 (13.5) years. Median contact delay time was 65 [150] min. Median transfer delay time was 28 [81.75] min. Median TPD was 120 [226.3] min: women, 120 [180] min and men, 119.5 [277.5] min. There was greater variability in delay times among men, as indicated by the wider interquartile range. Other delay times are shown in the Figure, although no statistically significant differences were observed (P=.483). Likewise, there were no significant differences by gender when the data were examined by time bands (Table).

Total Prehospital Delay Times in Acute Myocardial Infarction
| Times | Total | Women | Men | P |
| <1 h | 82 (22.2) | 41 (21.8) | 41 (22.5) | ns |
| 1-2 h | 100 (27) | 50 (26.6) | 50 (27.5) | ns |
| 2-6 h | 107 (28.9) | 61 (32.4) | 46 (25.3) | ns |
| >6 h | 81 (21.9) | 36 (19.1) | 45 (24.7) | ns |
| Total | 370 (100) | 188 (100) | 182 (100) |
ns, not statistically significant.
Data shown are no. (%).
With respect to the type of AMI, TPDs were significantly higher in non-Q wave AMIs (median, 166 min vs 108.5 min; P<.05) than in Q wave AMIs, due to the longer contact delay time (median, 75min vs 60min; P=.067); the transfer delay time was almost identical (median, 27min vs 28min; P=.759) in both genders.
The multivariate analysis was performed with variables identified by earlier studies2 as being associated with TPD and which were found to be significant, i.e. educational level (odds ratio [OR]=2.4; P=.001), pain intensity (OR=0.828; P=.003), history of ischemic heart disease (OR=1.871; P=.028) and diabetes at the limit of statistical significance (OR=1.686; P=.059).
In this study, in which patients were matched by age, we found no differences by gender in the time to seeking health care. Although sex matching is useful to control for a possible confounding effect of age, delay times in the overall sample were overstated for males. In contrast to our findings, most studies performed to date1,2,4 have reported longer delays in women. We believe that the difference may be due to the effect of age and sex. As reported in other studies,1,2,4 the difference by sex in delay times increases with age. The TPD in our study was 120min, which is comparable to that in other international studies.5 Surprisingly, despite technological advances in transportation over recent years, delay times have remained constant over the past 3 decades.5 Only half of patients reach the hospital within 120min after the onset of infarction pain, i.e. within the time considered appropriate in clinical practice guidelines6 if maximum benefit is to be obtained from reperfusion therapies. Delays could be reduced by educational campaigns to help patients recognize the early signs and clinical symptoms of AMI, particularly in groups with longer delay times such as diabetics or patients with low education levels.
FundingFondo de Investigación Sanitaria (PI06/90378).
.