The description and detailed evaluation of the extent and distribution of diseases, while recognizing their specific epidemiological and etiological characteristics, are important for establishing strategies to improve the health of the general population.1,2 Disease burden measures the health losses in the population that represent the fatal and nonfatal consequences of diseases and their risk factors. Specifically, the Global Burden of Disease study was the first to establish a standardized measure for measuring premature mortality (years of life lost [YLL]), a component of the synthetic indicator disability-adjusted life-years, which allows assessment of changes in the health of the general population.1–3 We used a classification of disease burden based on an etiological perspective, grouping the codes of the International Classification of Diseases (ICD) into different groups and categories in order to study disease burden. From this perspective, within the category of cardiovascular disease, heart failure (HF) as an underlying cause of death is included in the so-called garbage codes or ill-defined codes.1,4
Applying the methods described in the Global Burden of Disease study, we quantified the potential impact of deaths coded as HF on calculation of YLL due to cardiovascular disease in 2008 in Spain. Mortality data were obtained from anonymized microdata files from the Spanish National Institute of Statistics for deaths coded to ICD-10 codes: I50 (I50.0, I50.1, and 150. 9). The denominators were obtained from the current population estimates published by the Spanish National Institute of Statistics. Proportional reallocation was conducted by age and sex for deaths assigned to the ill-defined codes group (ICD-10, group R). The YLL attributed to HF were calculated by age and sex groups taking the Princeton West model life table (level 26 modified) as the reference.1 Social values (age-weighted [?=1] and the discount rate [3%]) were included, as proposed in this methodology.1 All calculations were performed using the GesMor software package.
In 2008, there were 126 252 deaths from cardiovascular diseases, of which 17% were attributed to HF (5% of total deaths in Spain). The crude mortality rate due to HF was 46/100 000 (31.6 men and 60.0 women) and rate adjusted to the standard European population was 23.6/100 000 (22.6 men and 23.3 women). Of the total YLL due to cardiovascular disease (504 091), 12% (60 339) were attributed to HF (9% men and 16% women). The proportion of YLL assigned to HF in relation to all cardiovascular diseases increased with age and was higher among women than men in all the age groups studied, reaching 24% of women =85 years (Table).
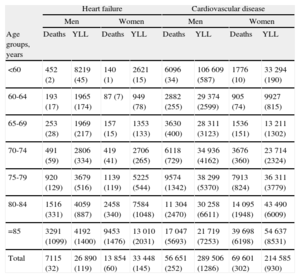
Total Number of Deaths, Crude Death Rates, and Years of Life Lost Due to Heart Failure and Cardiovascular Disease by Age and Sex. Spain, 2008
| Heart failure | Cardiovascular disease | |||||||
| Men | Women | Men | Women | |||||
| Age groups, years | Deaths | YLL | Deaths | YLL | Deaths | YLL | Deaths | YLL |
| <60 | 452 (2) | 8219 (45) | 140 (1) | 2621 (15) | 6096 (34) | 106 609 (587) | 1776 (10) | 33 294 (190) |
| 60-64 | 193 (17) | 1965 (174) | 87 (7) | 949 (78) | 2882 (255) | 29 374 (2599) | 905 (74) | 9927 (815) |
| 65-69 | 253 (28) | 1969 (217) | 157 (15) | 1353 (133) | 3630 (400) | 28 311 (3123) | 1536 (151) | 13 211 (1302) |
| 70-74 | 491 (59) | 2806 (334) | 419 (41) | 2706 (265) | 6118 (729) | 34 936 (4162) | 3676 (360) | 23 714 (2324) |
| 75-79 | 920 (129) | 3679 (516) | 1139 (119) | 5225 (544) | 9574 (1342) | 38 299 (5370) | 7913 (824) | 36 311 (3779) |
| 80-84 | 1516 (331) | 4059 (887) | 2458 (340) | 7584 (1048) | 11 304 (2470) | 30 258 (6611) | 14 095 (1948) | 43 490 (6009) |
| =85 | 3291 (1099) | 4192 (1400) | 9453 (1476) | 13 010 (2031) | 17 047 (5693) | 21 719 (7253) | 39 698 (6198) | 54 637 (8531) |
| Total | 7115 (32) | 26 890 (119) | 13 854 (60) | 33 448 (145) | 56 651 (252) | 289 506 (1286) | 69 601 (302) | 214 585 (930) |
YLL, years of life lost.
Data are expressed as No. (rate per 100 000 population).
The proportion of deaths due to cardiovascular causes assigned to HF in Spain is higher than that observed in other countries such as the US (6%), Mexico (8%), and Brazil (10%).4 Several factors may contribute to these differences, such as the quality of completing death certificates, the autopsy rate, and epidemiological differences. Determining HF etiology is not always easy but is easier in ischemic heart disease than in other heart diseases such as hypertensive heart disease. Therefore, a higher prevalence of ischemic heart disease, as observed in other countries or in men and younger age groups, may help to at least partly explain the lower percentage of deaths assigned to the HF in these population groups.
Despite the recommendation of the World Health Organization that HF should not be assigned as the underlying cause of death, this entity represents a large proportion of cardiovascular mortality in Spain. Given that the main causes of HF in Spain are ischemic and hypertensive heart disease,5,6 the use of mortality statistics to calculate YLL may considerably underestimate premature mortality due to these 2 specific causes, an effect that is more marked in the case of women.
Finally, understanding the epidemiology of HF and its risk factors is of great importance to implement interventions and programs that can control its impact on the health of the general population. Thus, efforts should be maintained and intensified to conduct and document an etiologic diagnosis during the patient's life and to improve the quality of completing the death certificate, so that, whenever possible, the cause is included and an ICD code is assigned to the underlying cause of death.
FUNDINGThe authors received research grants from the Fondo de Investigación Sanitaria, Instituto de Salud Carlos III (Project PS09/086).
NoteThe results of this study were presented at the XXX Scientific Meeting of the Spanish Society of Epidemiology (Santander, October 17-19, 2012) and the European Congress of Epidemiology (EUROEPI 2012; Oporto, September 5-8, 2012). The opinions expressed in this letter are the responsibility of the authors and do not necessarily reflect the views of the organizations for which they work.
.