Although the number of patients requiring a heart transplant has remained stable in our setting, the time on the transplant waiting list has lengthened. This has increased implantation of long-term left ventricular assist devices (LVADs) in patients with end-stage heart failure.1 However, when the cause is hypertrophic cardiomyopathy (HCM) or restrictive cardiomyopathy, mechanical support is not a clear-cut option because the anatomical characteristics associated with these conditions are usually considered a contraindication for LVAD therapy.2,3 The left ventricle is often too small or trabeculated, which implies a risk of collapse while on support, insufficient circulatory assistance with low output, suction of surrounding tissue, thrombosis, and stroke.2,3 Optimizing flow without creating suction becomes even more complex when the patient begins to move and change position because of changes in the orientation of the inlet cannula. For these reasons, HCM patients seldom receive LVADs, and studies on the topic include small, single-center series that have even included both hypertrophic and restrictive cardiomyopathy patients.2,3 We present the case of an HCM patient in our hospital who received an LVAD, the first indicated in Spain. The objectives were to confirm that selected patients can benefit from this therapy and to provide information on the anatomic, functional, and surgical parameters that may be useful for LVAD implantation in patients with HCM.
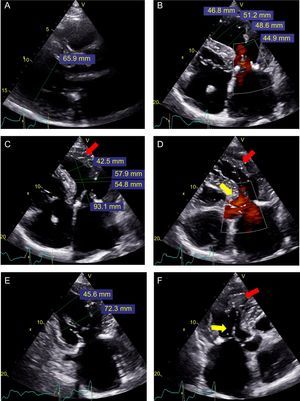
The patient reported is a 66-year-old man with obstructive HCM, who underwent defibrillator implantation in 2004 following resuscitation from an episode of sudden death due to ventricular fibrillation. In 2013 he was treated with septal ablation, which was unsuccessful. He was admitted for heart failure in 2015, and was referred for pretransplantation evaluation. Three months later, after optimization of the medical and resynchronization therapy, he was included on the elective waiting list. After 1 year on the list, he developed irreversible pulmonary artery hypertension, and we opted to evaluate LVAD therapy a bridge to decision. Right heart catheterization (September 2016) showed right atrial pressure (RAP) at 11 mmHg; mean pulmonary artery pressure, 45 mmHg; pulmonary capillary wedge pressure (PCWP), 22 mmHg; cardiac index, 1.5 L/min/m2; and pulmonary vascular resistance, 9.2 UW. The RAP/PCWP ratio was 0.45 and the right ventricular (RV) stroke work index was 397 mmHg/mL/m2. Transthoracic echocardiography was performed (Figure 1) to evaluate the RV and its dimensions, which seemed sufficient. The patient had grade III/IV mitral regurgitation due to anterior systolic movement and a dynamic outflow tract gradient of 50 mmHg, with no aortic regurgitation. The basal RV diameter was 48 mm, tissue Doppler S’ was 9cm/s, tricuspid annular plane systolic excursion (TAPSE) was 14 mm, radial function was preserved on subjective evaluation, and the fractional area change was 59%. Transesophageal echocardiography ruled out intraventricular thrombi and shunts. The relevant analytical results were creatinine clearance, 53mL/min and N-terminal probrain natriuretic peptide, 4.866 pg/mL. The calculated HeartMate II score was 2.67.
. B: Apical 4-chamber view in systole; various diameters from the base (44.9 mm) to the apex (46.8 mm). C: Apical 4-chamber view in diastole; various diameters from the base (54.8 mm) to the apex (42.5 mm); trabeculation in the lateral apical region (red arrow), not seen in systole. D: Apical 4-chamber view in systole and in color; trabeculation in the lateral apical region (red arrow), with better definition of the separation with the lateral wall; the yellow arrow shows acceleration in the outflow tract. E: Apical 2-chamber view in end-diastole; end-diastolic diameter of the basal (72.3 mm) and middle (45.6 mm) left ventricle. F: Apical 3-chamber view in systole; anterior systolic movement (yellow arrow) and apical trabeculation (red arrow) are observed.")
Transthoracic echocardiogram before implantation. A: Parasternal long axis view; left ventricular end-diastolic diameter (65.9 mm). B: Apical 4-chamber view in systole; various diameters from the base (44.9 mm) to the apex (46.8 mm). C: Apical 4-chamber view in diastole; various diameters from the base (54.8 mm) to the apex (42.5 mm); trabeculation in the lateral apical region (red arrow), not seen in systole. D: Apical 4-chamber view in systole and in color; trabeculation in the lateral apical region (red arrow), with better definition of the separation with the lateral wall; the yellow arrow shows acceleration in the outflow tract. E: Apical 2-chamber view in end-diastole; end-diastolic diameter of the basal (72.3 mm) and middle (45.6 mm) left ventricle. F: Apical 3-chamber view in systole; anterior systolic movement (yellow arrow) and apical trabeculation (red arrow) are observed.
In October 2016, a HeartWare HVAD system was implanted, with 113 min of on-pump circulation. The need for additional surgical procedures was ruled out. Septal myectomy was considered unnecessary, as it would make the surgery more complex and require aortic clamping with a risk of subsequent aortic regurgitation or residual shunts. Transesophageal echocardiography was used during the procedure to visually confirm that the apical trabeculae did not interfere with the inflow orifice of the system. Resecting the trabeculae is technically difficult as it is done through the small orifice made by coring the ventricular apex. By obviating this procedure, there would be no remnants from incomplete resection that could be suctioned by the LVAD. At the pump outlet, the RV was supported with milrinone and adrenaline, and nitric oxide was used to reduce the afterload. Nitric oxide discontinuation was rapidly achieved, with extubation at 9hours. Low-flow events occurred in the first 24 to 48 hours, despite the low support (2400 rpm). These responded to preload optimization by fluid replacement to achieve an RAP of 10 to 12mmHg, mean blood pressure of 65 to 80mmHg, and gradual tapering of inotropic and vasopressor agents (milrinone and adrenaline). This last measure is important to resolve low-flow episodes by preventing the increase in left ventricular contractility secondary to inotrope use from causing the patient's ventricle to compete with the LVAD. In our patient, the RV responded well and it was easy to withdraw inotropic therapy relatively quickly. The patient was discharged with LVAD support optimized to 2500 rpm and 4 to 4.5 L/min, with no low-flow problems (Figure 2).
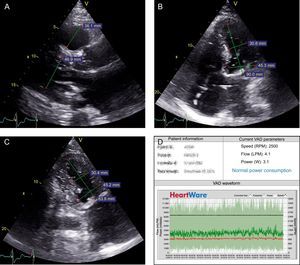
, right ventricular diameter (36.1 mm at this level). B: Apical 4-chamber view; end-diastolic diameter of the basal (45.3 mm) and middle (31 mm) left ventricle. C: Apical 2-chamber view; end-diastolic diameter of the basal (45.2 mm) and middle (30.4 mm) left ventricle. D: HeartWare HVAD programming; normal parameters with circadian rhythm and no low-flow events. LPM, liters per minute; RPM, revolutions per minute; W, watts.")
A–C: Transthoracic echocardiogram following implantation. A: Parasternal long-axis view; left ventricular end-diastolic diameter (46.9 mm), right ventricular diameter (36.1 mm at this level). B: Apical 4-chamber view; end-diastolic diameter of the basal (45.3 mm) and middle (31 mm) left ventricle. C: Apical 2-chamber view; end-diastolic diameter of the basal (45.2 mm) and middle (30.4 mm) left ventricle. D: HeartWare HVAD programming; normal parameters with circadian rhythm and no low-flow events. LPM, liters per minute; RPM, revolutions per minute; W, watts.
In conclusion, LVAD therapy is possible in patients with HCM, particularly those in the dilated phase, and it could be an additional option in patients with relative contraindications for transplantation. Nonetheless, selection of patients for this therapy is challenging and involves adjustments in preload, afterload, inotropism, and the LVAD support parameters.