To the Editor:
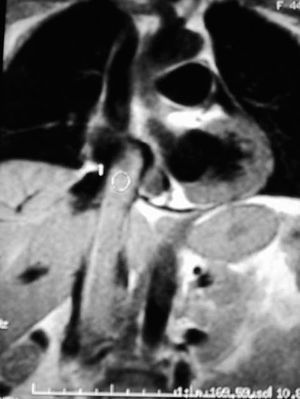
Intravenous leiomyomatosis is an uncommon benign tumor of the uterus that proliferates throughout the venous system, but does not invade it (Figure 1). Its treatment represents a surgical challenge requiring the coordination of several surgical teams. We describe the operative approach employed in a 44-year-old woman with this lesion and discuss the different surgical options.

Figure 1. Image showing the extension of the tumor in inferior vena cava and right atrium.
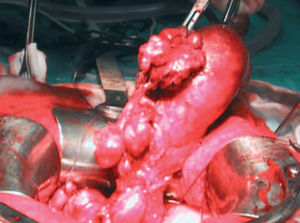
The operation involved a single procedure, carried out jointly by cardiovascular, peripheral vascular and gynecologic surgeons, via simultaneous midline sternotomy and laparotomy. First, hysterectomy with bilateral salpingo-oophorectomy was performed, followed by the establishment of cardiopulmonary bypass between ascending aorta and superior vena cava, involving the right appendage as well. After induction of deep hypothermia, circulatory arrest was maintained for 20 minutes (rectal temperature: 15ºC). With the 2 teams working simultaneously, right atrium, inferior vena cava, and left iliac vein were opened and the tumor was removed without difficulty (Figure 2). The postoperative period was uneventful and, four years later, the patient remained asymptomatic and presented no evidence of recurrence.

Figure 2. Intraoperative image of the together with the myomatous uterus.
Many techniques have been employed in the treatment of tumors of this type, as well as renal and adrenal tumors that invade the inferior vena cava and/or right atrium.1,2 Basically, they include resection carried out in separate surgical procedures or in a single operation involving combined midline sternotomy and laparotomy. Those who defend successive procedures argue that the operative time required to perform this surgery in a single operation is too long and increases the risk of bleeding owing to the systemic heparinization necessitated by cardiopulmonary bypass.3 The first surgical session, performed under cardiopulmonary bypass, would consist of the resection of the tumor, achieving its elimination up to the renal veins. In a second stage, control of the vena cava would be established in the infrarenal region, adequate venous return would be ensured and the risk of incomplete resection and of embolization would be lowered.4 The interval between the 2 operations varies from one report to another but, in view of the slow growth of the tumor, some groups waited up to 6 weeks to undertake the second stage.
The other surgical strategy consists of a combined abdominal and thoracic procedure involving cardiopulmonary bypass, with circulatory arrest and deep hypothermia.5 We have found this approach to be safe in tumors of this type. It permits the removal of the tumor in a single operation, in a bloodless operative field, which facilitates the proper excision of the lesion with minimal preliminary manipulation of the inferior vena cava and the heart, manipulation that favors intraoperative embolization. The operative time is not excessively prolonged, since the tumor is usually easily removed. The increased risk of bleeding presented as an argument by those who defend the two-stage procedures was not especially notable in our case. Circulatory arrest with deep hypothermia avoids subjecting the liver and kidneys to periods of warm ischemia. Other advantages of this technique are the physical benefits for the patient and economic benefits for the system, as the surgery is performed in a single operation. We are of the opinion that a multidisciplinary surgical approach is of fundamental importance for the proper management of this lesion.
In view of the low incidence of embolism and the limited number of adhesions involved, some authors propose employing only laparotomy in the removal of tumors of this type.6 In our opinion, this approach should be avoided as it can pose a threat due to possible tumor emboli, lesions in vessels in which vascular control has not been achieved and the risk of an incomplete resection. A right atrial approach should be avoided for the same reasons. Deaths due to retroperitoneal exsanguination have been reported.