

Coronary microvascular dysfunction (CMD) is highly prevalent and is recognized as an important clinical entity in patients with coronary heart disease (CHD). Nevertheless, the association of CMD with adverse cardiovascular events in the spectrum of CHD has not been systemically quantified.
MethodsWe searched electronic databases for studies on patients with CHD in whom coronary microvascular function was measured invasively, and clinical events were recorded. The primary endpoint was major adverse cardiac events (MACE), and the secondary endpoint was all-cause death. Estimates of effect were calculated using a random-effects model from published risk ratios.
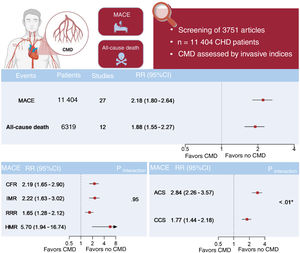
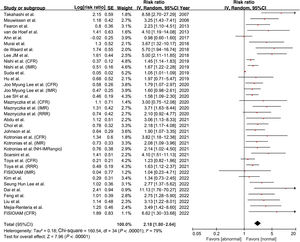
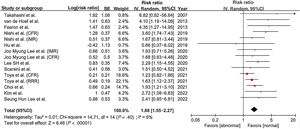
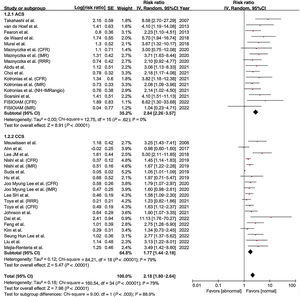
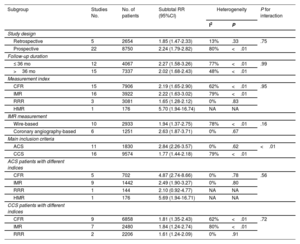
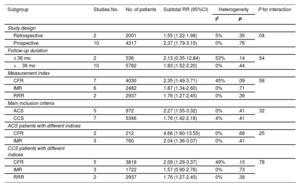
ResultsWe included 27 studies with 11 404 patients. Patients with CMD assessed by invasive methods had a higher risk of MACE (RR, 2.18; 95%CI, 1.80-2.64; P<.01) and all-cause death (RR, 1.88; 95%CI, 1.55-2.27; P<.01) than those without CMD. There was no significant difference in the impact of CMD on MACE (interaction P value=.95) among different invasive measurement modalities. The magnitude of risk of CMD assessed by invasive measurements for MACE was greater in acute coronary syndrome patients (RR, 2.84, 95%CI, 2.26-3.57; P<.01) than in chronic coronary syndrome patients (RR, 1.77, 95%CI, 1.44-2.18; P<.01) (interaction P value<.01).
ConclusionsCMD based on invasive measurements was associated with a high incidence of MACE and all-cause death in patients with CHD. The magnitude of risk for cardiovascular events in CMD as assessed by invasive measurements was similar among different methods but varied among CHD populations.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm