Keywords
The middle aortic syndrome with localized or diffuse stenosis of the inferior thoracic aorta or the abdominal aorta is an unusual cause of arterial hypertension in the upper extremities.1 This syndrome may be caused by Takayasu disease,2 usually diagnosed by angiography, which shows stenosis of the affected segments. We present the case of a 13-year-old girl with involvement of the aorta and renal arteries, treated with renal balloon angioplasty and stent implantation in several segments. Follow-up 2.5 years later was documented by computerized helicoidal tomography images with contrast.
CLINICAL CASE
A 13-year-old girl was admitted to our hospital with severe cardiac insufficiency and basal rales, hepatomegaly, and significant cardiomegaly. She was treated with diuretics, digital, and steroids, with rapid clinical improvement. During the examination, 160/70/95 mm Hg hypertension was found in the upper extremities associated with weak femoral pulses and a systolic murmur in the back. Cardiac catheterization was performed under general anesthesia, by accessing a vein to the aorta with 5 Fr Multipurpose and Pigtail catheters. Angiographic study revealed a stenotic segment in the thoracic aorta, located in the diaphragm, 8 cm long by 5 mm in diameter (Figure 1A) and other severe stenosis of the abdominal aorta (3 mm in diameter) between the origin of the renal arteries and the iliac bifurcation, without opacification of the iliac or left femoral arteries (Figure 2A). Selective injection of contrast material revealed additional stenosis in the right renal artery (Figure 3). A peak to peak systolic gradient of 45 mm Hg in the thoracic aorta and 35 mm Hg between the proximal and distal abdominal aorta were observed, as was a 40 mm Hg gradient of the right renal artery.

Fig. 1. A: Aortogram reveals a large stenotic segment in the thoracic aorta located in the diaphragm.

Fig. 2A. Aortogram reveals stenosis of the abdominal aorta between the origin of the renal arteries and the iliac bifurcation. The left iliac artery is not visible.

Fig. 3. Right renal arteriogram that shows stenosis at it origin.
All clinical and angiographic data confirmed the diagnosis of Takayasu disease affecting the mid-aorta. Some of these lesions were initially treated with therapeutic catheterization. Heparin at a dose of 100 U/kg was administered to the patient. Angioplasty with a 4 mm diameter Tacker balloon at 20 atm pressure was performed on the stenosis of the right renal artery, with clear improvement obtained. Later, an 8 Fr Mullins catheter was introduced into the right femoral artery and 3 Palmaz stents (P-308 Johnson & Johnson) were implanted to dilate the stenotic segments of the mid and descending aorta. Two superimposed implanted stents were expanded sequentially in the diffuse stenosis of the diaphragm (Figure 1B), utilizing a Powerflex 10 mm diameter by x 4 cm long balloon for its implantation and dilatation. The third stent was implanted in the stenosis of the abdominal aorta (Figure 2B), using a similar balloon measuring 8 mm in diameter by 4 cm long. Immediately following the implant, the aortic pressure gradient disappeared, achieving a decrease in systemic arterial pressure (from 210/160/180 to 140/90/105 mm Hg). The superior stenotic segment diameter increased from 5 to 10 mm and the inferior diameter from 3 to 8 mm. After the procedure, acetylsalicylic acid at a dose of 5 mg/kg was administered for 3 months.

Fig. 1.B: Aortogram after the implantation of 2 superimposed stents.

Fig. 2B. Aortogram after the implantation of the stent in the stenotic segment of the abdominal aorta. Very severe stenosis of the left iliac artery is seen.
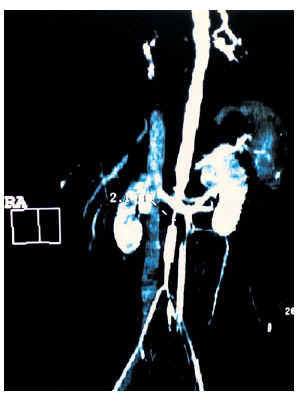
Immunodepressor treatment with steroids and azatoprine was initiated for treatment of Takayasu disease that continues to the present time. A general improvement in hypertension was achieved (130/80/98 mm Hg, associated with nifedipine and enalapril treatment) with better exercise tolerance. At 6 months, the child´s parents refused a repeat catheterization to re-dilate the stents. Instead, computerized helicoidal tomography with contrast was performed at 1- and 2-year-followup, and similar results were obtained on both studies. The images confirmed the permeability of the stents and revealed a new, very severe, area of stenosis just below the renal arteries (Figure 4). At present, the patient is in a good state of health, with arterial pressure of 121/55 mm Hg, according to the latest Holter monitor, and continues with enalapril and nifedipine treatment.

Fig. 4. Computerized helicoidal tomography on which the permeability of the implanted stents can be seen, as can new stenotic segments in the abdominal aorta located in the renal arteries.
DISCUSSION
Aortic arteritis is a chronic inflammatory disease of unknown etiology that affects the aorta and its branches. In children, it is an aggressive and frequently lethal disease, with a mortality rate according to one study of 35% during 5-year observation period.3 The mechanical obstruction appears to be the predominant cause of hypertension in patients with significant stenosis in the aorta. Takayasu disease with congestive cardiac insufficiency has been found more frequently in children than adults.4 In these circumstances, the initial diagnosis may be difficult because of the absence of hypertension and weak peripheral pulses caused by congestive cardiac insufficiency.
The characteristic clinical picture (hypertension of the upper extremities with weak or absent femoral pulses) may, as in our patient, appear after initial treatment of cardiac insufficiency. The anatomy of the stenotic segments may reveal circumscribed or diffuse lesions located in the thoracic or abdominal aorta. Treatment consists of attempts to dilate with balloon in cases of localized stenosis4,5 or surgery, interposing a bypass with conduit when a very long segment is affected.2As in our patient, balloon angioplasty may be especially effective in decreasing circumscribed stenosis of the renal artery.6 In the case of diffuses aortic obstructions, there is a greater risk of uncontrolled dissection of the aortic wall or post-dilation re-stenosis, and implantation of stents may be more useful and provide greater treatment safety.7,8 In our patient, treatment was planned in stages and stents were electively dilated at a suboptimum diameter that was less than that of a normal aorta in the stenotic areas, in an attempt to avoid over-dilation. A decision to re-dilate at a later date was rejected by the child´s parents. Therefore, we were obliged to control the progression of the disease with helicoidal tomography with contrast and 3-dimensional image reconstruction. We had the same experience as Quanadil et al9 in the use of non-invasive monitoring in this disease. At medium-term follow-up, we detected disease progression in spite of continued immunodepressor treatment.
CONCLUSION
Our experience confirms that the mid-aorta syndrome caused by Takayasu disease progresses in severity. Stent implantation may be palliative, and continuous follow-up with computerized helicoidal tomography is necessary both short- and long-term.
Este trabajo ha sido realizado según el programa gubernamental de cooperación hispano-polaca.
Correspondence: Dr. J. Bialkowski.
41 800 Zabrze, Szpitalna 2. Polonia.
E-mail: jabi_med@priv4.onet.pl