
Percutaneous treatment of mitral regurgitation (MR) is an option for high risk patients who are not candidates for mitral valve surgery because of ventricular dysfunction1,2 or comorbidities. It has been shown to be a safe and effective technique.2,3
Patients selected for this procedure should fulfil certain anatomical criteria, which can largely be assessed by 2 -dimensional transesophageal echocardiography (TEE).3 However, 3-dimensional TEE makes it easier to assess the complex morphological and functional parameters of the mitral valve, as well as changes after mitral valve percutaneous repair.4
Anatomical mitral valve requirements for MitraClip deployment are quite strict and include central regurgitant jet origin (scallops A2-P2).3 Two-dimensional TEE is not always able to precisely identify the originating location.
The aim of our study was to analyze mitral valve anatomic regurgitant orifice (ARO) using 3-dimensional TEE and its association with reduced regurgitation following MitraClip implantation.
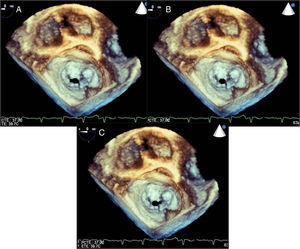
The study design was a case series. Patients with significant MR were consecutively enrolled from November 2011 to September 2013 if they fulfilled anatomical criteria assessed by 2-dimensional TEE for MitraClip (Abbott Vascular) implantation. We excluded patients with an eccentric origin of regurgitant jet. We studied ARO morphology using 3 -dimensional TEE (Philips iE33), classifying cases as purely central (C) if A2-P2 was affected alone, or central-eccentric if the segments adjacent to A2-P2 were affected, in which case they were subclassified as central-medial (CM) or central-lateral (CL) (Figure).

We assessed the association between ARO morphology and MR reduction (grades 1–4)3 and the absence of immediate reduction following device deployment. An optimal result was considered as a final MR grade of 2 or less.
All variables were collected prospectively. Our series consisted of 20 patients. The device could not be deployed in 1 patient due to severe mitral stenosis. Two other patients were excluded due to organic MR and eccentric location of the regurgitant jet. Finally, 17 patients were included (mean age, 61 [SD, 16] years, 70% men; 59% functional class III according to the New York Heart Association; mean logistic EuroSCORE 14.78 [SD, 12]; mean left ventricular ejection fraction 28%; 88% had pulmonary hypertension). All patients had functional MR. The procedure was successful in all patients; 1 device was implanted in 14 patients and 2 were implanted in 3 patients. A complete 2- and 3-dimensional TEE study was performed pre- and postimplantation, and MR encompassed 4 grades.3–5 Informed consent was obtained.
Qualitative variables are expressed as an absolute number and percentage. Quantitative variables are expressed as mean (standard deviation). Student's t test was used to analyze the association between variables for independent or paired data, as appropriate. We used the software package PASW v.18. Significance was defined as P < .05.
After analyzing the results, we found that there were no significant differences between patients when grouped by baseline echocardiographic parameters (Table).
Echocardiographic Parameters
| Total (n = 17) | Group A (n = 6) | Group B (n = 11) | P | |
| Dd baseline, mean (SD), mm | 67.53 (10.86) | 63.33 (13.32) | 70.20 (8.10) | .22 |
| Sd baseline, mean (SD), mm | 55.46 (11.93) | 52 (14.49) | 58.30 (9.71) | .31 |
| EDV baseline, mean (SD), mm | 255 (91.64) | 232.83 (95.88) | 268.30 (91.46) | .47 |
| ESV baseline, mean (SD), mm | 183.68 (78.30) | 162.17 (89.49) | 196.60 (72.64) | .41 |
| LVEF baseline, mean (SD), % | 28.56 (12.45) | 34.33 (18.64) | 24.72 (5.35) | .12 |
| PASP baseline, mean (SD), mmHg | 47.87 (10.42) | 45.83 (13.76) | 48.72 (8.13) | .59 |
| TAPSE baseline, mean (SD), mm | 15.40 (4.25) | 16.20 (4.15) | 15.27 (4.33) | .69 |
| S wave baseline, mean (SD), cm/s | 9.24 (1.71) | 10.20 (1.75) | 8.67 (1.48) | .08 |
| MR grade baseline | 3.94 | 4 | 3.90 | .65 |
| ERO baseline, mean (SD), cm2 | 0.49 (0.06) | 0.46 (0.04) | 0.51 (0.07) | .12 |
| 3D-ARO baseline, mean (SD), cm2 | 0.43 (0.03) | 0.45 (0.02) | 0.43 (0.04) | .14 |
| 3D-VC baseline, mean (SD), cm2 | 0.42 (0.04) | 0.43 (0.03) | 0.43 (0.04) | .99 |
| AP mitral annulus diameter baseline, mean (SD), mm | 28.84 (5.11) | 27 (4.33) | 30.72 (5.19) | .16 |
| IC mitral annulus diameter baseline, mean (SD), mm | 41.31 (4.51) | 41.17 (5.38) | 42.18 (4.16) | .67 |
| MR grade final, mean (SD) | 1.7 (1.04) | 0.66 (0.51) | 2.27 (0.78) | <.0001 |
| ERO, final, mean (SD), cm2 | 0.20 (0.10) | 0.10 (0.06) | 0.25 (0.09) | .002 |
| Change in MR grade, mean (SD) | 2.24 (1.04) | 3.33 (0.52) | 1.63 (0.78) | <.0001 |
| Change in ERO, mean (SD), cm2 | 0.29 (0.12) | 0.36 (0.09) | 0.23 (0.10) | .048 |
3D-ARO, anatomic regurgitant orifice measured by three-dimensional echocardiography; 3D-VC, vena contracta measured by three-dimensional echocardiography; AP, anterior-posterior; Dd, diastolic diameter; EDV, end-diastolic volume; ERO, effective regurgitant orifice; ESV, end-systolic volume; IC, inter-commissural; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; PASP, pulmonary artery systolic pressure; Sd, systolic diameter; SD, standard deviation; TAPSE, M-mode tricuspid annular plane systolic excursion.
The ARO was purely central in 6 patients (group A) and was central-eccentric in 11 (group B). Mitral regurgitation was significantly reduced throughout the series (P < .0001) when assessed using both the semiquantitative method (reduction in MR grade) and the quantitative method (reduction in effective regurgitant orifice). When analyzed by group, the reduction was greater in group A (P < .0001), although there were no differences in the number of devices (1 patient in group A had 2 devices and 2 patients in group B had 2 devices; the remaining patients had 1 device).
As far as we are aware, there is no study in the literature that has analyzed MR reduction after MitraClip deployment using 3-dimensional TEE-assessed ARO morphology. Our results suggest that 3-dimensional TEE may well play a fundamental role in selecting ideal candidates for MitraClip treatment, at least in patients with functional MR. Furthermore, knowledge of ARO morphology may lead to changes in the location of device implantation (usually in the medial region between A2-P2), which may in turn improve outcomes. Similarly, other authors have found that 3-dimensional TEE contributes to a lower rate of postimplantation complications and an improved outcome.6
The results of this study should be interpreted with caution because of the small sample size. However, they show that regurgitant orifice morphology analyzed with 3-dimensional TEE is associated with a reduction in the degree of functional mitral regurgitation in patients treated with MitraClip.