To the Editor:
Mycotic aneurysms are rare and potentially lethal if not diagnosed early: it is the total infection of the arterial wall.1 Epidemiology changes and although bacterial endocarditis was originally the principal cause, it currently presents in older patients with atherosclerosis. Staphylococcus aureus,2Salmonella, and gram-negatives are the germs most frequently involved although in immunodeficient patients and intravenous drug-users any opportunist germ can be found.3,4 Seeding generally occurs on a diseased intima by direct contact with an adjacent focus of infection or by hematogenous or lymphatic dissemination.
Symptoms are highly nonspecific and patients often present a septic condition that is difficult to control and clinical manifestations related with early aneurysm rupture and rapid expansion, acting as local mass compressing adjacent structures.3,4
The diagnosis should be based on clinical suspicion and imaging techniques such as angiography and computerized tomography (CT), the technique of choice.3-5
We present the case of a young immunodeficient patient presented to our clinic with fever and cough, intense expectoration, continuous chest pain extending to the left shoulder with characteristics typical of pleuropericarditis.
In the physical examination he appeared in poor health with a temperature of 39°C, 30 respirations/minute tachypnea, 150 beats/minute tachycardia and blood pressure 120/70 mm Hg with absence of paradoxical pulse. We observed jugular venous distension when reclined at 45 degrees, as well as a pericardial friction rub and hypophony in the right base.
The electrocardiogram revealed an atrial flutter at 140 beats/minute. Chest x-rays showed bilateral alveolar infiltration and grade II global cardiomegaly. Transthoracic echocardiography showed grade II pericardial effusion without hemodynamic deterioration in the right cardiac cavities. The valves were structurally and functionally normal without lesions indicating endocarditis. The root of the aorta and the ascending aorta were normal.
Following initial diagnosis of respiratory infection and associated pleuropericarditis we started treatment with wide spectrum antibiotics. At 10 days post-admission, we found no improvement in symptoms and modified the treatment after detecting 2 S aureus positive blood cultures.
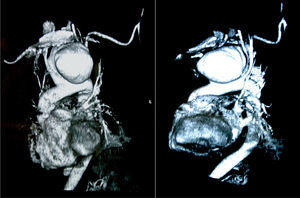
The x-ray showed progressive mediastinal thickening and helicoidal CT (Figure 1) identified a 10x13 cm saccular aneurysm in the aortic arch that compressed and displaced the left carotid artery, right brachiocephalic trunk and aortic arch.

Figure 1. Aortic arch aneurysm shown by helicoidal CT.
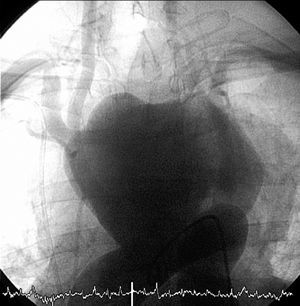
On confirming the presence of the aneurysm thru aortic angiography (Figure 2), the patient presented extensive ischemic stroke with abrupt diminution of level of consciousness and right hemiparesis. Initially, surgical intervention was not considered and the patient died 24 hours later, with strong suspicion of aneurysm rupture.

Figure 2. Aortic angiography.
To summarize, we are dealing with an immunodeficient patient with initial symptoms of pneumonia, pleuropericardial infection, atrial arrhythmias and symptoms of sepsis, who did not respond to treatment. Following x-ray evidence of mediastinal thickening, CT confirmed the presence of a large saccular aneurysm in the aortic arch. Aortic angiography was performed to determine the exact location of the aneurysm neck and its anatomic relationship with the aorta branches.4,5
We suspected the aneurysm was caused by infection for two reasons: the presence of symptoms of sepsis with S aureus positive blood cultures, which favors the seeding of germs in the diseased intima, and rapid growth and expansion4 of the aneurysm, evolving to early rupture, which is a frequent characteristic of mycotic aneurysms.
In conclusion, mycotic aneurysms are rare and diagnosis is based on adequate clinical suspicion,2 imaging tests to detect aneurysm as early as possible, and a positive microorganism blood culture as confirmation. Antibiotic treatment3 should be started following initial diagnosis of suspicion and surgery is the immediate definitive treatment.1-4