
Keywords
INTRODUCTION
The leading cause of death in industrialized countries is cardiovascular disease (CVD), followed by cancer and respiratory diseases. Together, these three account for almost 75% of all deaths. The latest available data1 for our area of Catalonia, in northeastern Spain, show the main causes of death in men to be tumors, cardiovascular and respiratory diseases, external causes, and digestive and mental diseases; in women they are cardiovascular diseases, tumors, respiratory diseases, mental diseases, digestive diseases, and nervous system diseases. In both men and women, therefore, the most important causes of death are tumors and CVD. However, whereas tumors are the leading cause of death in men, in women they are the second cause.
Cardiovascular disease is an especially important cause of death in persons over 65 years of age. Within this group, coronary disease is more frequent in men and in persons aged between 65-74 years, whereas stroke is the most common cause in women and in all persons over the age of 75 years.
In the period covering 1999-20002 the most common tumor in men was lung cancer, with a mortality rate of 87.6 per 100 000 inhabitants, and in women it was breast cancer, with a mortality rate of 31.0 per 100 000 inhabitants. The main cause of cardiovascular death in men was ischemic heart disease, with a mortality rate of 104.4 per 100 000 inhabitants, and in women it was cerebrovascular disease, with a mortality rate of 96.8 per 100 000 inhabitants.
A study of the evolution of mortality in Catalonia from 1983-19923 showed an increase in the annual number of deaths (approximately 707) as a result of the aging of the population. By sex, the increase was slightly greater in men than in women (109 men for every 100 women, a ratio which remained stable throughout the whole study period). Life expectancy rose during the study period but it was not the same for both sexes; in 1983 the life expectancy for women was 5.79 years more than for men, and in 1997 this difference was 6.55 years.
Different patterns of mortality compared with the general population have been reported in certain groups of workers, especially those employed in the chemical industry, mainly as a result of exposure to certain components with possible cancerigenous effects. However, the excess risk and the magnitude of the difference vary considerably, depending on the study.4 These differences may be due to the progressive introduction of safety measures in this type of industry, tending to reduce the associated serious effects.
In Spain, few studies have been undertaken of patterns of mortality in working populations followed over a long period of time. A prospective, observational study was started in 1968 of a cohort of 1059 men aged 30-59 years, all workers in a factory making tires in the town of Manresa, situated in Catalonia in northeast Spain. The cohort was followed for 28 years, with periodic re-examinations every 5 years, the last in 1996. The aims of this present study were to describe the patterns of mortality of this cohort of workers followed for 28 years, assess the possible changes and compare the patterns with those of the general population.
SUBJECTS AND METHOD
Study Population
Manresa is a town in the county of Bages, which in 1968 had a population of 58 101 inhabitants. The study included all healthy male employees and workers aged 30-59 years at an important factory in Manresa manufacturing tires. The total number of participants was 1059 out of the 1084 who were eligible. This group was followed for 28 years. A detailed description of this cohort has already been published elsewhere.5 Importantly, the only criteria for leaving the study throughout the whole 28 years of follow-up were death during this period or loss to follow-up.
Baseline and Follow-up Examinations
The initial examination was undertaken in 1968, with repeat examinations every 5 years during the follow-up (1973, 1978, 1983, 1988) and in 1996. Detailed information concerning cardiovascular risk factors and other factors determined at the initial examination and during the follow-up examinations have been reported previously.5 The present study also included information regarding smoking and place of work, that is either in an administrative area or in the production area.
All episodes giving rise to periods of sick leave longer than 3 weeks were recorded and investigated. Data concerning any illnesses requiring hospitalization were obtained during the follow-up from the clinical charts at the health centers. The sick leave certificates and hospital records also provided useful information regarding death and causes of death.
The main source of information regarding death was the official death certificate, with additional information provided by the cause of death report from the insurance company. The factory had contracted life insurance policies for its workers. When the death of a worker occurred the insurance company physician issued a report, which was used to corroborate and validate the information on the official death certificate.
Data for those workers who had retired were obtained directly from the family or the reports of the Social Security physicians. Although retired workers left the factory and had no further dealings with it, they were still observed for the purposes of this study. Thus, data regarding the vital status of these retired workers and their diseases were obtained from the primary care physicians and the hospital of Manresa. The specific causes of death were classified according to the eighth revision of the international code for the period 1975-79 and the ninth revision thereafter.
Statistical Analysis
Rates were calculated for total mortality, death from cancer, and death from CVD, with person-years of follow-up as the denominator. The standardized mortality ratio (SMR) was calculated with PAMCOMP.6 The expected number of cause-specific deaths was calculated using the rates of male mortality for Catalonia for specific age groups,7 information which was available from 1975 on. Associations were calculated between the risks of death from any cause, from cancer and from CVD, and smoking habit and place of work, using the Cox proportional risk model. This model included age as a covariable with the introduction of smoking and place of work (administrative or non-administrative area). The statistical analyses were done with SPSS 11.0.
RESULTS
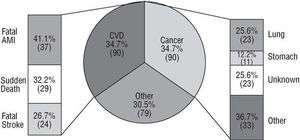
Table 1 shows the main characteristics of the study population. More detailed information concerning this population has been previously reported.5 Notably, of the 1059 participants at the start of the study, 49.1% were aged from 30-39 years, 32.3% from 40-49 years, and 18.6% from 50-59 years. At the first health examination, 67% of the workers were smokers and at the last examination 13.3% were smokers. Information was obtained for 96.4% of all the participants throughout the whole study period. Information concerning vital status was obtained for all participants at the end of the 28 years observation period. Those participants who failed to attend their last examination were contacted directly if possible or else by means of questioning a close relative about the participant's vital status. The cause of death was ascertained in all cases where the participant had died. The total number of deaths in the cohort was 259 (24%). The leading causes of death were CVD and cancer, with 90 (35%) deaths each (Figure 1).


Fig. 1. Description of the causes of death. CVD indicates cardiovascular disease; AMI, acute myocardial infarction.
Myocardial infarction was the most important cause of death within the group of CVD, followed by sudden death and stroke, with 37, 29, and 24 cases, respectively. The main cancers leading to death were lung cancer (23 cases) and stomach cancer (11 cases), followed at some distance by the other cancers. The type of cancer was not mentioned on the death certificate of 23 persons.
Table 2 presents the crude relative risk (RR) and the 95% confidence interval (CI) for death from lung cancer associated with smoking status at the start of the study and with place of work. The risk of death from lung cancer was two-fold greater in smokers compared with non-smokers and two-fold greater in labor workers compared with administrative staff. In no case, though, was the association significant. Multivariate analysis with Cox proportional hazards model showed that the RR of death from lung cancer associated with smoking was 2.4 (95% CI, 0.8-7.2), after adjusting for age and place of work (Table 2).

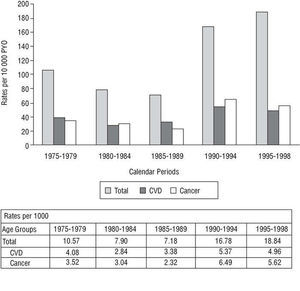
The trends in the patterns of mortality over the 28 years showed a slight drop in overall mortality between 1975-79 and between 1985-89, thereafter increasing in 1990-94 and 1995-98. The pattern of mortality was also different in these periods. After 1990 the rates of death from cancer were much higher than the rates of death from CVD (Figure 2).

Fig. 2. Mortality rates according to the calendar periods from all causes, cardiovascular disease, and cancer. CVD indicates cardiovascular disease; PYO, person-years observation.
No excess mortality was detected in this cohort in comparison with the general population. The SMR for overall mortality was 67.7% (95% CI, 59.7%-76.5%), for death from cancer the SMR was 84.3% (95% CI, 67.8%-103.6%), and for death from CVD the SMR was 100.5% (95% CI, 80.8%-123.6%) (Figure 3).

Fig. 3. Observed/expected deaths per calendar period. CVD indicates cardiovascular disease; CI, confidence interval; SMR, standardized mortality ratio.
Table 3 shows the specific rates of mortality according to age, cancer, CVD, and all-causes. The table also shows the corresponding numbers of observed deaths and expected deaths according to the mortality pattern for men in Catalonia during the same periods. Finally, as can be seen, the overall SMR according to age was approximately 50% lower than expected in the age groups of 60 years or above.

During the first 3 periods the overall mortality was much lower than expected from the figures for the general population. Death from CVD was also lower, whereas death from cancer was similar. During the last 2 periods, however, overall mortality, death from CVD and death from cancer were all similar to that expected. This pattern appears to correspond to the so-called "healthy worker effect," which means that actively employed persons are healthier than the general population. The rate of overall mortality in our study was lower than that for the general population because of a lower mortality rate during the first observation periods. The rate of cardiovascular death was slightly lower during the first periods, but overall the rate was similar to the expected rate, whilst the rate of death from cancer was similar to the expected rate during the first periods and slightly higher at the end of the study, with the overall rate just below the expected rate.
DISCUSSION
The Manresa study is the first prospective study in Spain of a cohort of workers observed over a long period of time. The population in question is ideal for carrying out epidemiological studies because it is a closed population with very little or no movement of labor, controlled over time and with almost no losses to follow-up. The results of the Manresa study show a similar pattern of mortality to that of the general population for the same period of time,3,8 with overall mortality rates lower than or the same as, but never higher than those of the general population. The main causes of death were CVD and cancer.
As with the general population, the results of this study also showed an increase in death from cancer over the last few decades and a slight reduction in death from CVD. The rate of death from CVD in Spain rose up until the mid 1970s,9,10 after which it has decreased slowly but constantly. This reduction began with women and was later seen in men. The reduction in absolute mortality in Catalonia has been greater in men, although it has also been seen in women over recent years.11
The death rate from cancer, however, rose progressively in Catalonia to peak in the 1990s, at which time it became stable and then began to decline slowly.12 Lung cancer has been the leading cause of death from cancer in men over the last decades. The most notable increase occurred between 1981-90, after which the rate stabilized and then fell until 1998. This pattern of death closely resembles the pattern for the European Union, comparing the period 1975-79 with 1990-94, the last period for which published data are available. The death rate reported in the Manresa study underwent a similar increase to that seen in other countries in southern Europe.13
Smoking could account for the progressive increase in cancer, more pronounced in men. The fact that smoking accounted for no more than 5% of deaths in our study may be due to the small sample size of persons with events. The decreasing trend in cardiovascular death, however, could be due to the identification of different cardiovascular risk factors and their subsequent control, as well as improvement in the early treatment of CVD.14,15 This reduction in the number deaths is very important, especially considering the high rate of CVD. Nevertheless, despite the fall in the number of deaths from coronary disease, the number of persons with the disease continues to rise, although at a slower rate now after a period of rapid increase.
Although the patterns of mortality in our study were the same as those for the general population, overall mortality was 30% lower than expected. This difference may be due to the "healthy worker effect". A study published in 200016 reported the rates of mortality over 8 years in healthy male workers and compared them with persons who did not participate in the study and with the general population. The healthy worker effect was shown by the fact that the active workers had constantly lower rates of mortality than those of the general population.
The possible effect of rubber on death rates has been studied by others. A systematic review published in 1998 analyzed the cancerigenous effect of rubber.4 The conclusion was that most studies showed a moderate increase in the risk of cancer of the bladder, larynx, and lung and also an increase in leukosis, although the magnitude of the association varied considerably. Recent studies, however, have provided specific information about the lack of increase in the risk of cancer with exposure to rubber, although the preventive measures taken by the industry over recent years could explain the reduction in the risk. A study published at the end of 1998 reported on a retrospective cohort of 15 649 male workers involved in the treatment of rubber, for whom information had been collected about death and the cause of death.17 The study found an excess risk of death from leukemia, but not from other types of tumor. No increased risk of cancer was detected in the workers in our study, either overall or after adjusting for smoking and place of work. Nor was there an increase in death from CVD, as has recently been reported.18 However, the interpretation of the results of this latter study and the conclusions have been subject of controversy.19
In conclusion, this study shows that the main causes of death were CVD and cancer in this cohort of workers who were followed-up over 28 years. The leading cause of death from CVD was acute myocardial infarction, with lung cancer being the most common cause of death from cancer. The rates of mortality according to the calendar periods changed over time, with an increase in de at h from cancer during the last period. The healthy worker effect could be seen in this cohort, which had a similar pattern of mortality to that of the general population, but with a lower overall mortality, due to a lower number of deaths during the first years of the study compared to the number of expected deaths according to the male population from Catalonia with the same age range.
Correspondence: Dra. T. Puig Reixach.
Servei d'Epidemiologia Clínica i Salut Pública.
Casa de Convalescència, 4.a planta.
Hospital de la Santa Creu i Sant Pau.
Sant Antoni M. Claret, 171. 08041 Barcelona. España.
E-mail: tpuig@hsp.santpau.es