




The CHA2DS2-VASc score, used to assess the risk of left atrial appendage thrombus (LAAT) formation in patients with atrial fibrillation (AF), has limited predictive value. Moreover, transesophageal echocardiography imaging, the gold standard diagnostic method to identify thrombi, is semi-invasive. Consequently, there is a need for alternative and noninvasive diagnostic methods for LAAT risk assessment.
MethodsDeep proteomic analysis was conducted in plasma samples from 8 patients with nonvalvular AF, divided into thrombus and control groups (4 patients in each group) based on the presence or absence of LAAT. Biomarkers associated with LAAT were validated using an enzyme-linked immunosorbent assay in a cohort of 179 patients with available clinical, transthoracic, and transesophageal echocardiography data. Predictive models were developed to assess the improvement in LAAT identification.
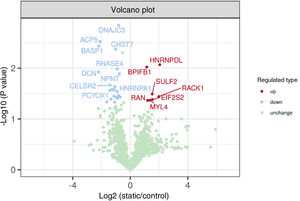
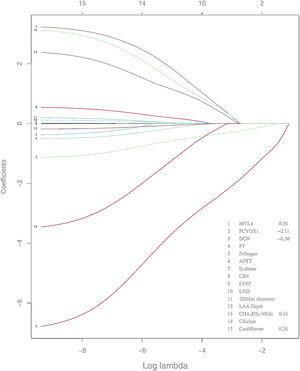
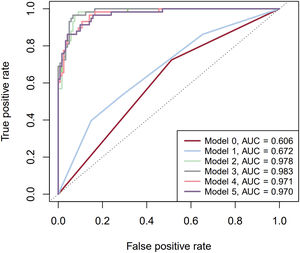
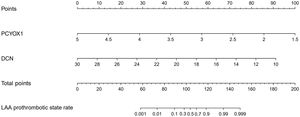
ResultsThe LAAT group had higher CHA2DS2-VASc scores, larger LA diameter, and lower LAA flow velocities. Deep proteomic analysis identified 30 differentially expressed proteins, including myosin light chain 4, prenylcysteine oxidase 1 (PCYOX1), and decorin as potential diagnostic biomarkers of LAAT. The model showed that PCYOX1 and decorin provided an area under the curve (AUC) of 0.970 for LAAT prediction compared with 0.672 in a model including the CHA2DS2-VASc score and LAA cauliflower morphology. The incremental value of proteomic biomarkers for LAAT in patients with nonvalvular AF was further confirmed with the net reclassification improvement and integrated discrimination improvement indices.
ConclusionsProtein levels of PCYOX1 and decorin improve the predictive performance for LAAT in patients with nonvalvular AF.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm