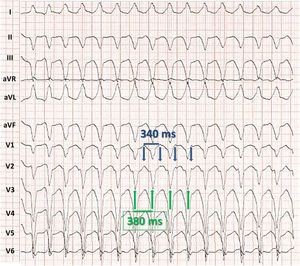

Several criteria can be used to support diagnosis of ventricular tachycardia and rule out aberrant supraventricular tachycardia: the presence of atrioventricular (AV) dissociation (evident in V1), RS> 100ms in precordial leads,1 and Q wave> 40ms in aVR2 (response 1, incorrect). Likewise, the presence of AV dissociation rules out antidromic tachycardia (response 2, incorrect). Analysis of the duration of the atrial activity cycle in V1 (figure 1, blue arrows) shows that this is shorter than the ventricular activity (green arrows), thus ruling out the possibility that atrial activity is due to retrograde ventriculoatrial conduction (response 3, incorrect). Therefore, the correct answer is number 4. As shown in figure 2, the patient's baseline rhythm is atrial flutter of typical appearance, with paced QRS and onset of an episode of ventricular tachycardia after the fourth paced beat. This confirms that 2 tachycardias are present, a typical flutter and sustained monomorphic ventricular tachycardia.
ISSN: 1885-5857
Impact factor 2024
4.9

