While in sinus rhythm, the patient had a PR interval of 120ms and an apparently preexcited QRS, with a positive delta wave in inferior and precordial leads. During atrial fibrillation, there was no change in the QRS with respect to baseline, which ruled out a conventional accessory pathway (between the atrium and ventricle).
The preexcitation is explained by the presence of an accessory pathway inserted beneath the atrioventricular node, which connected the specific conduction system to the ventricle (fasciculoventricular). The onset of atrial fibrillation did not alter the QRS, as the atrioventricular node continued to “filter” the conduction of impulses to the ventricles.
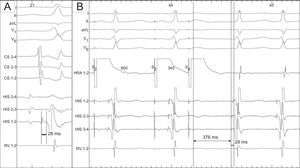
The electrophysiological study (Figure) revealed an HV interval of 28ms (normal, between 35 and 55ms), a finding that confirmed the suspicion of preexcitation (Figure A). The patient had nodal reentrant tachycardias (Figure B) unrelated to the presence of the fasciculoventricular pathway (accessory pathways of this type do not participate actively in tachycardias).1
