
We report a percutaneous transfemoral aortic valve implantation (TAVI) procedure in a patient with infrarenal saccular abdominal aortic aneurysm (SAAA) treated by endovascular surgery during the same procedure.
We present the case of an 82-year-old man, with a history of smoking, adenocarcinoma of the colon treated by surgery and adjuvant chemotherapy in the previous 6 months, and SAAA extending to both iliac arteries with maximum diameters of 69×57 mm in multiplane reformat on computed tomography), admitted for non–ST-segment elevation acute coronary syndrome and left heart failure. Echocardiography showed a very calcified aortic valve and severe stenosis, with valve area of 0.88 cm2, peak and mean gradients of 71.7 mmHg and 35 mmHg, respectively, and mild left ventricular hypertrophy with normal ejection fraction. Catheterization showed coronary artery disease with a large obstructive lesion in the proximal left anterior descending artery. The patient had a logistic EuroSCORE of 19.06%. The medical-surgical team decided to treat the diseased artery and aortic stenosis using a percutaneous approach and the SAAA by endovascular repair.
During the first procedure, a conventional stent (Stent Vision 3.5×23 mm; Abbot Vascular, Santa Clara, California, Unites States) was implanted in the proximal left anterior descending artery via the right femoral artery, without complications and with a good angiographic result.
Three weeks later, a second procedure was performed with the patient under general anesthesia. After both femoral arteries were exposed, an abdominal aortic stent and the aortic valve (Edwards-SAPIEN XT 26; Life Sciences, Irvine, California, United States) were implanted. The vascular surgeon began the percutaneous procedure with exclusion of the SAAA, achieved by placing a bifurcated stent with extensions into both iliac arteries. Final angiographic control showed that there were no leaks and minimum diameters of 10 mm were obtained in both iliac arteries (Figure 1).

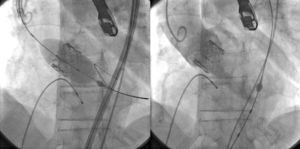
Subsequently, TAVI was performed via the left femoral artery following standard procedures, with a good final outcome and mild residual paravalvular regurgitation (Figure 2). The procedure ended with surgical closure of both femoral arteries.

At 6 months after implantation, the patient remained asymptomatic from the cardiological point of view. Computerized tomography showed that there were no leaks from the aortic stent.
To our knowledge, this is the second published case1 of simultaneous transfemoral TAVI and endovascular repair of an SAAA. In our case, abdominal aortic stent implantation was followed by TAVI, whereas in the first study TAVI was followed by abdominal aortic stent implantation using the same guidewire.1
One other TAVI procedure in a patient with a previously surgically implanted ascending aortic stent has been described in the literature.2
We decided to perform the procedure in this sequence for 2 reasons: first, to avoid dissections caused by advancing the TAVI devices, and second, because it is known that after prosthetic valve implantation there is an increase in blood pressure that increases the risk of dissection or abdominal aortic aneurysm rupture if SAAA repair is delayed. In these cases, the only precaution to be taken after SAAA repair is that the introducer sheath used in the TAVI procedure should be advanced through the implanted aorto-iliac stents via the less tortuous femoral artery, making sure that that this is done slowly, with no sudden movements, and under angiographic guidance to avoid stent deformation or displacement from the implantation site.
Age and comorbidities led us to simultaneously perform both procedures, although we acknowledge that SAAA is an off-label indication for TAVI via the femoral artery (several TAVI procedures with off-label indications are described in the literature2,3). An alternative route such as the subclavian artery was not used because endovascular aneurysm repair was needed due to the high risk of rupture of the SAAA needing endovascular repair.
This case highlights the importance of coordinated efforts by a multidisciplinary team that includes cardiologists, vascular surgeons, anesthesiologists, and interventional cardiologists to manage these conditions that are increasingly found in elderly patients.