A patent ductus arteriosus (PDA) in the third day of life is a physiologic shunt in healthy term and preterm newborn infants. In contrast, hemodynamically significant PDA is a common complication for very preterm or very small infants with high morbidity and mortality, affecting more than 40% of preterm infants.
Several comorbidities are associated with PDA, such as necrotizing enterocolitis, intraventricular hemorrhage, pulmonary edema/hemorrhage, chronic lung disease, and retinopathy of prematurity. Standard therapy for PDA closure has predominantly involved surgical ligation, indomethacin, and ibuprofen. The mechanism of action for both indomethacin and ibuprofen is through inhibition of prostaglandin synthesis, resulting in ductal constriction. Both drugs appear to be equally effective in closing echocardiographically confirmed PDA. The optimal timing for treatment remains controversial.1
Several adverse events have been reported with these drugs, including peripheral vasoconstriction, gastrointestinal bleeding and perforation, decreased platelet aggregation, hyperbilirrubinemia and renal failure.
Paracetamol acts by directly inhibiting the activity of prostaglandin synthase. The role of paracetamol as an alternative treatment for the closure of PDA is under investigation.1,2
The results of using paracetamol to treat PDA in 3 preterm infants are shown in the Table.
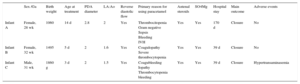
Clinical Characteristics and Echocardiography Findings of Patients Treated With Endovenous Paracetamol
| Sex /Ga | Birth weight | Age at treatment | PDA diameter | LA:Ao | Reverse diastolic flow | Primary reason for using paracetamol | Antenal steroids | SO4Mg | Hospital stay | Main outcome | Adverse events | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Infant A | Female, 28 wk | 1060 | 14 d | 2.8 | 2 | Yes | Thrombocitopenia Gram negative Sepsis Bleeding IVH | Yes | Yes | 170 d | Closure | No |
| Infant B | Female, 32 wk | 1495 | 5 d | 2 | 1.6 | Yes | Coagulopathy Severe thrombocytopenia | Yes | Yes | 39 d | Closure | No |
| Infant C | Male, 31 wk | 1860 g | 3 d | 2 | 1.5 | Yes | Coagubleeding Iopathy Thrombocytopenia bleeding | Yes | Yes | 39 d | Closure | Hypertransaminasemia |
AO, aorta; GA, gestational age; LA, left artery; PDA, patent ductus arteriosus; SO4Mg, magnesium sulfate.
Infant A was a 28-week gestational age (GA) girl weighing 1060g (third monochorionic triplet) who was ventilated for respiratory distress syndrome. A large PDA was diagnosed on the 14th day of life. Ibuprofen and PDA ligation were contraindicated due to severe sepsis by Klebsiella sp, thrombocytopenia, and grade III intraventricular hemorrhage. Intravenous paracetamol was started at a dose of of 15mg/kg/4 times a day (QID) and PDA closure was achieved after 5 doses. Paracetamol was discontinued after 6 days. There were no adverse effects and the infant was discharged after 170 days.
Infant B was a 32-week GA preterm girl weighing 1495g. On the fifth day of life, a large PDA was diagnosed and, due to severe thrombocytopenia, paracetamol was started at a dose of 15mg/kg/ QID for 3 days. After 48hours, the ductus was closed with no adverse effects. The infant was discharged after 39 days.
Infant C was a 31-week GA preterm boy weighing 1860g. A large PDA was diagnosed and, because of severe thrombocytopenia and bleeding, intravenous paracetamol was started at a dose of 15mg/kg/QID for 3 days. Closure of the PDA was achieved after 48hours. Hypertransaminasemia was detected (glutamic oxaloacetic transaminase 2624U/L; glutamic-pyruvic transaminase 365 U/L) but normalized in the next 72hours. No other adverse effects were diagnosed. The patient was discharged at 39 days of life.
PDA can be treated effectively with intravenous indomethacin and ibuprofen, which are nonselective cyclo-oxigenase inhibitors and decrease prostaglandin synthesis, leading to permanent ductal closure in 60% to 80% of infants. Preterm infants treated with ibuprofen seem to have lower serum creatinine values, higher urine output, and fewer adverse effects than those receiving indomethacin. However, because of the potential adverse effects associated with both ibuprofen and indomethacin and patient instability in some cases, clinicians must look for alternative treatments and paracetamol could be used in these cases.
Paracetamol is used worldwide for its analgesic and antipyretic actions. Several studies have demonstrated the potential efficacy of paracetamol in early PDA. In 2011, Hammerman et al.3 reported the first case series of preterm infants and observed that oral paracetamol for a period of 3 days at a dose of 60mg/kg/QID was effective for closing PDA.
Two studies that enrolled 250 preterm infants and compared the effectiveness and safety of paracetamol vs ibuprofen concluded that the success rate of paracetamol for PDA closure was similar to that of ibuprofen with no more adverse events.4
El-Kuffash et al.5 reported late closure of PDA with intravenous paracetamol at a dose of 60mg/kg/day, divided in 4 doses. Oncel et al.6 reported the results of a randomized controlled trial in preterm infants treated with oral paracetamol in whom closure PDA was achieved with no complications.
Even though there are studies about paracetamol with different doses and routes of administration, due to the dire clinical situation of the patients in our study, we started intravenous paracetamol at a dose of 15mg/kg/QID for 3 days in infants B and C. The infant with the lowest GA (infant A) received paracetamol for 6 days. Infant A was also the patient in whom treatment was started after the second week of life. Despite the delayed treatment, PDA closure was achieved.
As reported by Hammerman et al.,3 severe thrombocytopenia was the most frequent reason for contraindicating ibuprofen.
According to the literature reported to date and our findings, hypertransaminasemia was the only adverse effect observed and no treatment was required.
Finally, paracetamol appears to be a promising new alternative to indomethacin, ibuprofen, and surgery for closing PDA with possibly fewer adverse events, although a limited number of infants have been studied. Nevertheless, in view of a recent report about adverse events on the developing brain of mice, long-term follow up to at least 24 months of postnatal age must be considered.
It is important to consider the possibility that paracetamol may be effective in the treatment of late PDA and could be an alternative to PDA ligation in patients with a contraindication to ibuprofen or indomethacin. The potential adverse effects of ibuprofen and indomethacin make paracetamol an attractive alternative pharmacological treatment.