Coronary artery bypass graft (CABG) is the treatment of choice in certain clinical and anatomical contexts in coronary artery disease, as described in clinical practice guidelines, including those of the European Society of Cardiology, which has been adopted by the Spanish Society of Cardiology.1
The aim of this study was to analyze the number of patients referred for CABG in our setting, determine the rate of interventions per head of population, compare the rate obtained with other rates in Spain, and appraise the degree of compliance with the recommendations of the clinical practice guidelines.
To achieve this, we determined the number of patients referred for CABG by our unit between January 1, 2012 and October 31, 2013, computed the number of patients treated per million inhabitants in our region, and compared these results with the situation in other parts of the country. Finally, we analyzed the number of patients who should have been referred for CABG according to the recommendations of the guidelines. Our unit is the provincial referral center for cardiac catheterization and has a catchment area of 630 000 inhabitants.
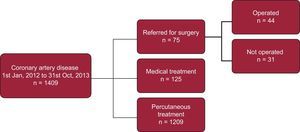
During the study period, severe coronary disease was diagnosed in 1409 patients. These patients’ therapeutic management is shown in the Figure. Of 75 referrals, 44 underwent surgery (58.7%), 27 (61%) underwent isolated CABG, and the remainder underwent combined CABG and valve replacement. This corresponds to 38.1 and 23.3/million inhabitants per year for combined surgery and isolated CABG, respectively. Thirty-one patients did not undergo surgery because they had died, had refused to undergo surgery, or because the cardiac surgeon did not consider them suitable for surgery, among other reasons.

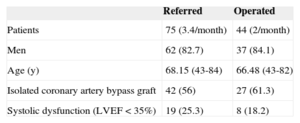
The clinical profile (Table) of the 42 patients referred for isolated CABG was absence of high surgical risk and high SYNTAX score (chronic occlusions, trunk disease and/or multivessel disease with multiple lesions). Referral was generally decided upon after consultation between the cardiac catheterization specialist and the clinical cardiologist.
Clinical Profile of Referred Patients Who Underwent Surgery
| Referred | Operated | |
|---|---|---|
| Patients | 75 (3.4/month) | 44 (2/month) |
| Men | 62 (82.7) | 37 (84.1) |
| Age (y) | 68.15 (43-84) | 66.48 (43-82) |
| Isolated coronary artery bypass graft | 42 (56) | 27 (61.3) |
| Systolic dysfunction (LVEF < 35%) | 19 (25.3) | 8 (18.2) |
LFEV, left ventricular ejection fraction.
Values are expressed as no (%) or mean (range).
According to the registry of interventions of the Spanish Society of Cardiovascular Surgery, 7149 patients underwent CABG in Spain in 2011 (154/million inhabitants per year); of these, 5010 underwent CABG only (111/million inhabitants per year) and the remainder combined surgery.2 In Germany in the same year, 55 299 patients underwent surgery (680/million inhabitants per year) and 41 976 underwent CABG only (516/million inhabitants-year).3 In the United States in 2010, isolated CABG was performed in 219 000 patients (697/million inhabitants per year).4
Because these data are influenced by the prevalence of the disease in different geographical areas, we analyzed the ratio between percutaneous revascularization and CABG. At our center, this ratio was 44.7 for isolated CABG and 24.7 for combined surgery. According to the Spanish Cardiac Catheterization Registry, 63 202 patients underwent percutaneous revascularization in 2011, giving a percutaneous revascularization/CABG ratio of 12.6 for isolated CABG and 8.8 for combined surgery.5 In the United States in 2010, the percutaneous revascularization/CABG ratio was 2.2.
Patients with multivessel disease are a heterogeneous group and it is difficult to generalize strategies;6 nevertheless, the clinical practice guidelines of the European Society of Cardiology1 clearly state that CABG is indicated in diabetic patients with disease in 2 or more vessels (class 1, level A). The number of patients who met this criterion in our study and who, according to the recommendations, were candidates for CABG as the first therapeutic option, was 287 (20.3%). CABG should also be considered in other anatomical contexts, such as main artery disease and multivessel disease with complex SYNTAX score, etc.
We believe that the results of this study are consistent with standard practice in Spain; while our data have the limitation of being from a single center, and one that does not have a cardiac surgery department, they indicate that CABG is used sparingly and that there is a lack of adherence to some of the recommendations of the European Society of Cardiology clinical practice guidelines on coronary revascularization, which have been adopted by the Spanish Society of Cardiology. Even if the comparison between our data and the general situation in Spain and other countries should not be considered rigorous because it relied on data from voluntary registries and did not include patients who, despite residing in our catchment area, were not treated at or referred from our center, the available information indicates that CABG is used to a lesser extent in Spain, and probably with significant regional differences.
Scientific societies for cardiology and cardiac surgery should appraise this situation, which, among other consequences, hampers cardiac surgeons’ ability to acquire and maintain new skills. If indeed there are specific circumstances that advise against applying the European guidelines in Spain, then we should develop our own national guidelines. Otherwise, we need to determine the causes that have created and continue to promote this attitude and develop measures to correct them.