To the Editor,
Paravalvular leaks occur in between 3% and 7% of cardiac valve prostheses. As many patients in whom closure is indicated are at high surgical risk, it is often necessary to resort to percutaneous techniques. Such approaches are complicated by the lack of specifically designed materials. Nevertheless, results continue to improve as a result of advances in imaging techniques and the development of new devices.
Anterograde or retrograde approaches can be used according to the location of the prosthesis and the leak. Despite the use of stiff guidewires or looped guidewires to establish arteriovenous loops, advancing the introducer for the dispensing catheter through the leak is usually the most complicated step.
We present a case in which a transapical technique1,2 was used when both anterograde and retrograde approaches failed. This new technique allowed rapid and straightforward access to the leak, as well as providing good support for advancement of the introducer.
The patient had aortic and mitral mechanical valve prostheses and had been admitted to hospital three times for acute pulmonary edema. A paravalvular leak estimated by transesophageal echocardiography (TEE) to be 8mm high, 6mm long, and 4mm wide was observed in the posteroseptal region and was associated with severe mitral insufficiency and signs of hemolysis. As the patient had a logistic EuroSCORE of 32%, a decision was taken to attempt percutaneous closure. The first attempt employed an anterograde approach via transeptal puncture. Despite the use of stiff guide wires, no catheters could be introduced that would allow positioning of the device. In the same procedure, a retrograde approach was also attempted. When the catheter was advanced to the left ventricle through the aortic valve prosthesis, one of the discs of the prosthesis was repeatedly blocked, leading to severe hemodynamic deterioration. A decision was therefore taken to attempt a transapical procedure.
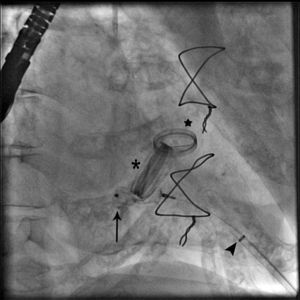
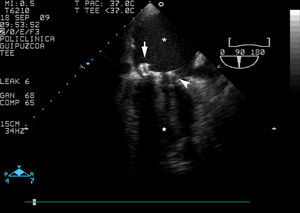
Forty-eight hours later, the procedure was done under general anesthesia with TEE guidance. After localization of the apex by transthoracic echocardiography, a left anterior minithoracotomy was performed and a tobacco pouch suture prepared. The apex was punctured with a trocar and a standard “J” 0.035mm guidewire (Bolton Medical Inc. Sunrise, FL, USA) was advanced to place an 8 French introducer (Terumo Medical Corp, Tokyo, Japan). A straight, hydrophilic, 0.035mm guidewire (Terumo Medical Corp, Tokyo, Japan) was advanced through the leak until it reached the left atrium and then a Vista Brite tip JR 3.5 catheter (Cordis, Miami, FL, USA) was advanced over it. The guidewire was then replaced with a stiff guidewire (Amplatzer Super Stiff. AGA Medical. Golden Valley, MN, USA) that allowed the 8 French catheter for the device to be advanced. A Vascular Plug III (AGA Medical. Golden Valley, MN, USA) occlusion device measuring 12mm×5mm was then advanced with the dispensing catheter in the left atrium and when only the distal segment had been opened it was withdrawn towards the left ventricle until it reached the leak, without releasing it. The mitral insufficiency disappeared but the device interfered with one of the discs and a decision was taken to remove the entire system. Another Vascular Plug III occluder measuring 12mm×5mm was advanced and, this time, it was opened completely in the left atrium before inserting it into the leak (Figure 1). The device did not interfere with any of the discs but left slight residual paravalvular insufficiency. After performing pushing maneuvers and confirming that it was well supported, the device was released (Figure 2). Finally, the tobacco pouch suture was closed.

Figure 1. Angiogram showing the device (arrow), introduced through the dispensing catheter via a transapical approach (arrowhead), along with the mitral valve prosthesis (asterisk) and the aortic valve prosthesis (star).

Figure 2. Transesophageal echocardiogram. The final position of the Vascular Plug III occlusion device (arrow) can be seen along with the mitral valve prosthesis (arrowhead), the left atrium (asterisk), and the left ventricle (star).
During follow-up, echocardiography and direct visualization did not reveal morphologic or functional changes compared with the results obtained immediately following implantation.
The patient was discharged and continued to show clinical improvement.
The transapical technique may speed up, facilitate, and simplify procedures for closure of paravalvular leaks and should be considered in complex cases or in those situations in which percutaneous approaches have failed.
Corresponding author. garikoitzll@hotmail.com