Coronary artery fistula draining into the left ventricle (CAF-LV) is a rare congenital heart disease, which increases the risk of myocardial ischemia, endocarditis, rupture of coronary artery aneurysm and so on.1,2 After surgical repair, residual shunt is not uncommon (17%).3 In comparison, transcatheter closure might become an alternative treatment, and its feasibility and effectiveness have been suggested in previous publications.4 However, group research and long-term follow-up are still absent after transcatheter closure of CAF-LV. This study was carried out to investigate its long-term outcome.
From January 2011 to September 2020, a total of 21 consecutive patients (15 men, 6 women, age 34.14±15.13 years) with CAF-LV were included according to guidelines on the management of congenital heart disease (with symptoms of a typical murmur),2 and transcatheter closure was performed successfully in all patients. The origin and drainage of CAF-LV were determined arteriographically, and the appropriate device was selected based on the minimum size and morphology of CAF-LV (figure 1A,B). Dual-antiplatelet therapy was employed in CAF-LV patients after transcatheter closure. Anticoagulant and antiplatelet therapy was selected by CAF-LV patients with a giant coronary artery aneurysm. Follow-up was performed by X-rays, 12-lead electrocardiogram and transthoracic echocardiography (TTE) records at 1 day, 1 month, and serially at 2- to 6-month intervals. The residual shunt measured by TTE was classified as follows: trivial (1mm), mild (1-2mm), moderate (2-4mm), or large (4mm). Clinical characteristics are shown in table 1. Among 21 patients, CAF-LV originated from the right coronary artery in 15 patients (71.43%), and there was 1 “recanalized” CAF-LV after surgical repair (figure 1C,D). Dilation of the feeding coronary artery was observed in 20 patients (95.24%), and “giant” coronary artery aneurysm was identified in 3 patients. In all, 37 devices was deployed, and the residual shunt was detected in 3 patients (trivial in 2 and mild in 1). After transcatheter closure, 10 patients experienced nonspecific ST-T wave changes. During the follow-up period (median, 2.83 years), there was a significant decrease in left ventricular end-diastolic dimension (52.24 ± 7.48mm vs 56.86 ± 11.39mm, P =.004). Six months after the intervention, 1 patient with giant coronary artery had a myocardial infarction (4.76%). In the remaining patients, no complications occurred during long-term follow-up.
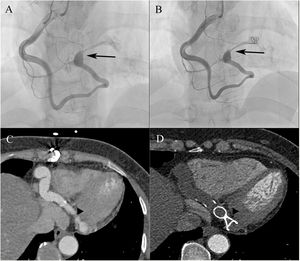
. B: the CAF-LV was occluded with an interlocking detachable coil (black arrow). C: MSCT showed the “recanalized” CAF-LV 8 years after surgery (arrowhead). D: the CAF-LV was occluded with a patent ductus arteriosus occluder (arrowhead). CAF-LV, coronary artery fistula draining into the left ventricle; MSCT, multislice computed tomography.")
Transcatheter closure of CAF-LV. A: arteriogram showing tortuous CAF-LV (black arrow). B: the CAF-LV was occluded with an interlocking detachable coil (black arrow). C: MSCT showed the “recanalized” CAF-LV 8 years after surgery (arrowhead). D: the CAF-LV was occluded with a patent ductus arteriosus occluder (arrowhead). CAF-LV, coronary artery fistula draining into the left ventricle; MSCT, multislice computed tomography.
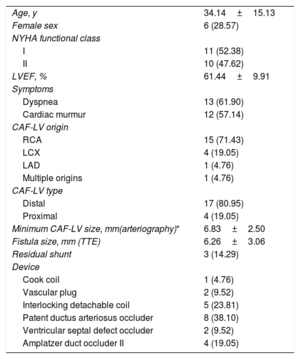
Clinical characteristics of patients with coronary artery fistula draining into the left ventricle (n=21)
| Age, y | 34.14±15.13 |
| Female sex | 6 (28.57) |
| NYHA functional class | |
| I | 11 (52.38) |
| II | 10 (47.62) |
| LVEF, % | 61.44±9.91 |
| Symptoms | |
| Dyspnea | 13 (61.90) |
| Cardiac murmur | 12 (57.14) |
| CAF-LV origin | |
| RCA | 15 (71.43) |
| LCX | 4 (19.05) |
| LAD | 1 (4.76) |
| Multiple origins | 1 (4.76) |
| CAF-LV type | |
| Distal | 17 (80.95) |
| Proximal | 4 (19.05) |
| Minimum CAF-LV size, mm(arteriography)* | 6.83±2.50 |
| Fistula size, mm (TTE) | 6.26±3.06 |
| Residual shunt | 3 (14.29) |
| Device | |
| Cook coil | 1 (4.76) |
| Vascular plug | 2 (9.52) |
| Interlocking detachable coil | 5 (23.81) |
| Patent ductus arteriosus occluder | 8 (38.10) |
| Ventricular septal defect occluder | 2 (9.52) |
| Amplatzer duct occluder II | 4 (19.05) |
CAF-LV, coronary artery fistula draining into left ventricle; RCA, right coronary artery; LCX, left circumflex coronary artery; LAD, left anterior descending coronary artery; NYHA, New York Heart Association; LVEF, left ventricular ejection fraction; TTE, transthoracic echocardiography.
Values are expressed as No. (%), or mean ± SD.
To the best of our knowledge, this is the first group research on transcatheter closure of CAF-LV. Our findings suggest that the long-term outcome was satisfactory in patients without giant coronary artery aneurysm, and that postoperative cardiac remodeling was favorable in most patients. In this study, the effectiveness of transcatheter closure was further confirmed, and there were 3 patients with trivial-mild residual shunt. During the long-term follow-up, myocardial infarction occurred in 1 of 3 patients with giant coronary artery aneurysm, which is consistent with a previous study.5 In CAF-LV patients with giant coronary artery aneurysm, it is difficult to predict postoperative myocardial ischemia, and further research is required to screen appropriate candidates.
FundingThis research was supported by the National Natural Science Foundation of China (81670283, 61975240).
Conflicts of interestNone declared.