To the Editor:
We are presenting a new case of thrombosis in the descending thoracic aorta of an apparently normal aorta, which is added to those previously reported.1 The subject is a woman, aged 50 with no previous medical or surgical background of interest. She arrived at the emergency service with a pain on her left costal margin. The chest x-ray revealed pleural effusion. A computerised tomography (CT) was performed, in which a mass was detected in the descending thoracic aorta measuring 6 cm in length and a width over 50% of the aortic calibre, indicative of a thrombus or tumour. A transoesophageal echocardiography (TOE) was performed in which no anomalies were detected on the aortic wall. The mass was distally anchored to the origin of the subclavian artery with a wide implantation pedicle and the rest floating freely in the descending aorta (Figure 1). Finally, a magnetic resonance imaging (MRI) with a contrast injection was performed, which showed a heterogeneous delayed enhancement of the mass (Figure 2).

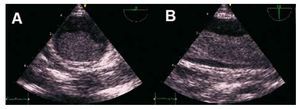
Figure 1. Transoesophageal echo-cardiography images. A: plane at 0º of the implantation base of the thrombus on the aortic wall, which presents slightly increased echogenicity. B: plane at 90º, which indicates the thrombus, mobile in the interior of the descending aorta.

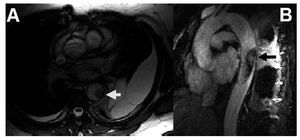
Figure 2. Magnetic resonance images. A: short axis cine-mode image, where the thrombus shows low signal intensity (arrow). B: maximum intensity reconstruction of the projection after administering contrast. Note the heterogeneous hyper highlight in the interior of the thrombus (arrow).
The pleural fluid analysis resulted in an exudate and pathological anatomy excluded the presence of malignant cells. The patient was surgically treated due to the persistence of the mass despite intravenous treatment with heparin. An aortotomy and a thrombectomy were performed. No significant alterations of the aortic wall were found and the anatomopathological diagnosis of the piece was thrombus. The patient was discharged feeling well on anticoagulant treatment awaiting the results of a full thrombophilia study.
We are aware of the long term evolution of our other 2 patients.1 The woman who required surgery remains asymptomatic under anticoagulant treatment. This patient also has a leukocytosis of uncertain significance, with a normal genetic study. The patient in which the dissolution of the thrombus with intravenous heparin was successful died 9 months later from a myocardial infarction from obstruction of the descending anterior artery, according to the necropsy results. This patient had followed a torpid course, determined by an undefined ileitis which required surgical resection a few months after suffering from aortic disease. All the malignancy and autoimmunity studies carried out had been negative.
This case poses new questions about this rare condition, about which a little over 100 examples have been published. Floating thrombi in the thoracic aorta are usually detected in elderly patients with diffuse atheroma in which the thrombus is anchored to an ulcerated plaque. However, they have also been described in a subgroup of a younger population, such as our patients, in the sixth decade of life. On occasions, it is possible to identify a remote closed thoracic trauma or a previous procedure of endovascular manipulation. However, in many other cases, no underlying cause is found and both the histology and the coagulability studies are normal. Other systemic factors could exist which induce a procoagulant state.2
The techniques for image diagnosis include TOE, CT, and MRI. The MRI is especially useful for the diagnosis and characterisation of intracardiac and intravascular masses. In differential diagnosis with MRI between thrombus and tumour, the contrast is more suggestive of a tumour. Nevertheless, chronic organised thrombi, can acquire neovascularisation and, are therefore enhanced after administering the contrast3,4 as in the case of our patient.
There are no reported series of cases that reflect the long term evolution of patients with floating intra-aortic thrombi without an underlying aortic disease. The characteristics of our patients indicate that the long term prognosis is not solely defined by the aortic appearance and the prevention of recurrences. The underlying cause, which manifests in a manner that is just as potentially serious in young patients with no other comorbidities may well be just as important, if not more so.