
We read the letter from J.A. San Román and I. Gómez Salvador and appreciate their interest in our study.
We understand the questions they raise regarding the association between variability and equity, but it is clear that therapeutic variability among similar populations within the same health system, when we are talking about therapies of proven efficacy and superiority, is an indicator considered to have a negative impact on quality of care and to directly affect equity.
The techniques assessed in our study have well-established evidence-based indications, which are reflected in the article, as the supplementary data includes a figure showing the classes of recommendations for each technique throughout the period.
It is important to remember that very similar studies were responsible for highlighting the considerable variation among European counties and regions in the implementation of primary angioplasty a few years ago (the Stent for Life initiative), leading to a definitive push to create infarct care networks throughout Spain and the rest of Europe.
The limitations of our study are clear, especially when you compare it to the ideal study, with ideal information sources, as in the editorial comment by Marrugat et al.1 on the subject. Our study used the best data available.
If our study serves to illustrate once more the need for high-quality registries of patients in a hospital setting, that would merge with regional registries that in turn would merge with national registries, we would be happy. The Swedish model is an example to follow.
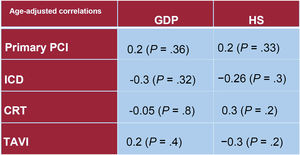
The authors of the letter appropriately commented on the effect of age. Obviously, the activity registries used in the study are not at a patient level, so it is not possible to adjust for characteristics such as age. However, many of the autonomous communities have similar population age profiles and, in any case, the scale of the variability in age between autonomous communities is not so wide as to explain, for example, the great difference in transcatheter aortic valve implantation.2 We have adjusted the correlation analysis between activity volumes and economic indices for mean population age of the autonomous communities during the period,3 and the significant correlation persists (figure 1).

Correlation adjusted for mean age of the autonomous communities. CRT, cardiac resynchronization therapy; GDP, gross domestic product per capita; HS, healthcare spending per capita; ICD, implantable cardioverter defibrillator; PCI, percutaneous coronary intervention; TAVI, transcatheter aortic valve implant.
We share the opinion that the guidelines are not a doctrine, but of course the recommendations should be adhered to as closely as possible, and any exception should be appropriately justified based on the clinical features of the individual patient.
FUNDINGNo funding.
AUTHORS’ CONTRIBUTIONSAll the authors participated with the following contributions: a) substantial contribution to the concept and design, data acquisition or analysis and interpretation; b) writing the article or providing critical review of its intellectual content; c) final approval of the version to be published, and d) accepting responsibility for all aspects of the article and agreeing to investigate and resolve any questions related to the accuracy and trueness of any part of the work.
CONFLICTS OF INTERESTThere are no conflicts of interest to declare.