

A 69-year-old man with very frequent supraventricular extrasystoles, functional class II, and mild ventricular dysfunction (48%) underwent an electrophysiology study. At baseline, he had dual antegrade atrioventricular nodal physiology (evidenced by an atrial-his [AH] jump), 2 echo beats, and dual nodal conduction (figure 1A, electrocardiogram; figure 1B, intracavitary recording during His-bundle sinus mapping with a high-density catheter; figure 1C, schematic representation and ladder diagram; A, right atrium; AVN, atrioventricular node; H, His; HP, His-Purkinje; V, right ventricle). As shown in figure 1B, atrial activation (A) caused 2 ventricular activations (V1 and V2) with a constant HV interval, both preceded by His-bundle activation (AH1fastpathway=125ms, AH2slowpathway=685ms, AH2-AH1=560ms). AH2 showed concentric retrograde atrial conduction with a short ventriculoatrial (VA) interval. The regularity of the His-His intervals distinguished them from His-bundle and atrioventricular junctional ectopics.

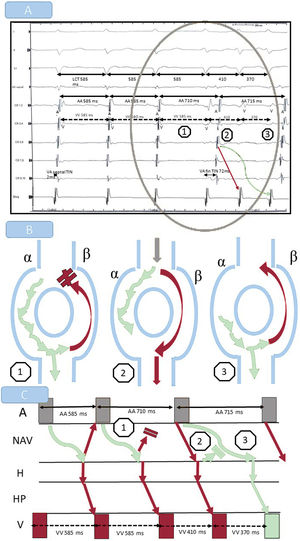
Isoproterenol induced spontaneous regular nonsustained narrow QRS tachycardia (rendering resetting or entrainment impossible) with a cycle length of 585 ms. Additional findings were concentric retrograde atrial activation with a VA interval of 2 ms; termination, probably due to retrograde block in the fast pathway (last tachycardia beat with a different VA interval, prolongation of the atrial-atrial interval, and no variations in the ventricular-ventricular interval); and restarting of dual nodal response (figure 2A, intracavitary recording with catheters in the septal right atrium, coronary sinus, and right ventricular apex; figure 2B, nodal conduction; figure 2C, ladder diagram). A septal accessory pathway was ruled out on demonstrating the retrograde Wenckebach phenomenon during ventricular pacing at a tachycardia rate. With a diagnosis of dual atrioventricular nodal nonre-entrant tachycardia and common nodal re-entrant tachycardia, the slow pathway was ablated, resulting in disappearance of the dual response, an improvement in functional class, and normalization of ventricular function.

The patient gave his consent for the publication of this case report.
FundingThis study received no funding.
Authors’ ContributionsD. Cantero Lozano: literature search, writing up of case report, and images. F. Rojas Simoni: noninvasive tests, clinical study, and contribution to case study. J. García-Fernández: electrophysiology study and writing up and revision of case report.
Conflicts of InterestThe authors have no conflicts of interest.