
To the Editor,
Mechanical alternans refers to the succession of strong and weak heartbeats. It is classically associated with advanced-stage heart failure although it can also be seen in aortic stenosis, hypertrophic cardiomyopathy, a sharp increase in cardio post load, a drop in preload, acute ischaemia and the onset of tachycardia. Mechanical alternans have been explained by mechanisms related to the Frank-Starling law, incomplete ventricular relaxation, partial asystole or variations in post load1 and, more recently, by disorders of the coupling between the release and re-uptake of calcium, supported by studies that found disorders in the genes of proteins related to calcium handling.2 Its negative impact on the prognosis of heart failure has been shown using the invasive measurement of dP/dt as the alternans pattern.1,2
We present the case of a patient with severe ventricular dysfunction in which alternans was recorded using the non-invasive measurement of dP/ dt according to the Bargiggia method.3
A 56-year-old male had inferoposterior myocardial infarction 3 years earlier. He has remained without angina, with class 2 dyspnoea treated with aspirin, enalapril, carvedilol, and statins. He came to the centre for an echocardiogram while in stable condition. The left ventricle was dilated (214 mL) with an ejection fraction of 29% (biplane Simpson method), with posterior dyskinesia and inferior akinesia, half-apical lateral and basal septal. He presented grade 2 mitral regurgitation (MR). There was no apparent right ventricular dysfunction and pulmonary systolic pressure was measured at 37 mm Hg.
Doppler recording of MR showed an alternating pattern with steeper and flatter curves (Figure 1) along the entire recording. The dP/dt was measured at 800 mm Hg/s for the steeper curves and 411 mm Hg/s for the flatter curves. The aortic ejection curve shows cyclical ventilation-related changes that disappear with apnoea (Figure 2A). Doppler tissue imaging in the lateral ring shows low systolic and diastolic velocities that vary from beat to beat (Figure 2B).

Figure 1. Recording of mitral regurgitation velocity using continuous wave doppler, showing the alternation of the slope from beat to beat.

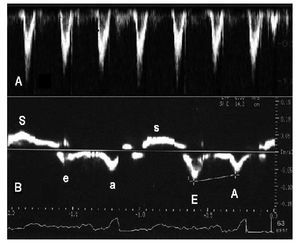
Figure 2. A: recording of aortic ejection flow using pulsed-wave doppler, showing a cyclical variation corresponding with the respiratory cycle, which disappears in apnoea. B: recording of lateral ring velocity using tissue doppler, showing beat-to-beat variations with larger waves (uppercase) and lower waves (lowercase), which affect systolic and diastolic velocities.
The Bargiggia method considers that the MR velocity permits measurement of the intraventricular systolic pressure by applying a modified Bernoulli's equation, making flow acceleration equal to the pressure generation velocity, dP/dt. To obtain dP/ dt, we measure the time that MR takes to accelerate from 1 to 3 m/s, corresponding to 4 and 36 mm Hg gradients, measuring dP/dt as the difference of the 2 gradients (32 mm Hg) divided by the time.3 This means that reducing the atrial pressure by equalising pressures and gradients and measuring an isovolumic phase parameter in patients in whom this does not exist. We can find cases where failure starts before the systole, as happens in the second beat in Figure 1, thus adding variability. Even with these limitations, this method of measuring dP/dt is closely correlated with the invasive value and is highly sensitive to changes in the inotropic state.3,4 Although it is essential that there be MR, it is common in patients with severe systolic dysfunction. Its use in studying alternans can be of great interest because it does not seem as affected by preload as is the aortic flow or the filling. It reflects overall ventricular function rather than an isolated segment and therefore eliminates the uncertainties brought about by tissue Doppler assessment, which although a useful technique for studying alternans,5 is affected by segmental contractility disorders and by ventilatory movements.