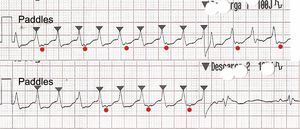
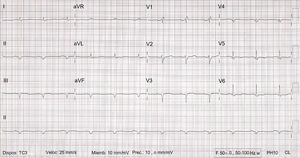
An initial R wave in aVR is a diagnostic criterion for ventricular tachycardia1 (response 1 incorrect). A QRS:P ratio of 1:1 is observed (more visible in aVL and V1); this is typical of supraventricular tachycardias, but more than 30% of ventricular tachycardias can show ventriculoatrial (VA) conduction2 (response 2 incorrect). Although the tachycardia did not resolve with amiodarone administration, retrograde conduction was reduced. Moreover, a VA ratio of 2:1 is observed in the rhythm strips (recorded after drug administration) (Figure 1, upper strip; P waves are marked with red circles) or occasional VA conduction (Figure 1, lower strip). The presence of more QRS than P waves practically confirms diagnosis of ventricular tachycardia (response 3 correct), supported already by the patient's history and QRS morphology in the ECG. The first electrical cardioversion of 100J was not effective (response 4 incorrect) but a second discharge of 150J did lead to resolution (Figure 1). Figure 2 shows the ECG after cardioversion.
ISSN: 1885-5857
Impact factor 2024
4.9

