
Heart transplant (HT) represents a major physiological stress, resulting in elevated levels of analytical biomarkers. This study aimed to determine whether changes in biomarker levels after HT can identify patients with a poor prognosis.
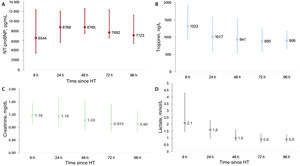
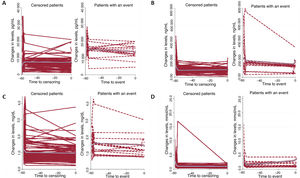
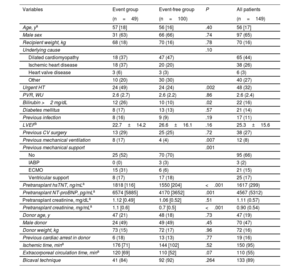
MethodsA prospective longitudinal noninterventional study was conducted in 149 consecutive patients undergoing HT from July 2017 to July 2023. Biomarkers were assessed before HT and at 6, 24, 48, 72, and 96hours after HT. The biomarkers analyzed were high-sensitivity troponin T, N-terminal pro-B-type natriuretic peptide (NT-proBNP), creatinine, and lactic acid. The primary outcome was a composite of death and severe primary graft failure (PGF).
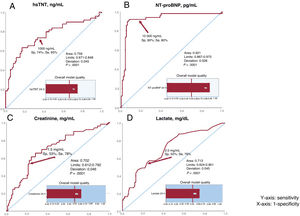
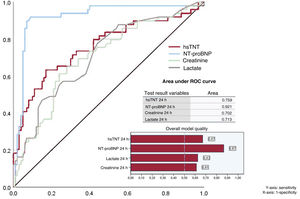
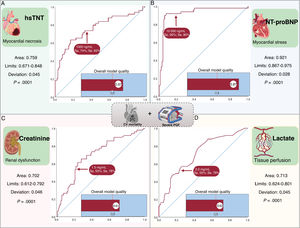
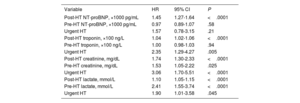
ResultsNT-proBNP and troponin levels remained highly elevated throughout the period and stabilized from the first 24hours post-HT. Lactate levels stabilized after the first 24hours, and creatinine from the second day onward. Exitus occurred in 23 (15%) of the patients, and severe PGF in 26 (17%). All biomarkers were significantly associated with the incidence of the combined event (P <.0001). Receiver operating characteristic curve analysis at 24hours showed significant areas under the curve (P=.0001). The greatest discriminatory power was observed for the NT-proBNP curve. A value of 10 000 pg/mL had a sensitivity of 90% and specificity of 80%.
ConclusionsA significant elevation of post-HT analytical biomarkers was associated with mortality and/or severe PGF. Among the biomarkers analyzed, NT-proBNP was the most accurate in classifying patients.
Keywords
Identify yourself
Not yet a subscriber to the journal?
")
Purchase access to the article
By purchasing the article, the PDF of the same can be downloaded
Price: 19,34 €
Phone for incidents
Monday to Friday from 9am to 6pm (GMT+1) except for the months of July and August, which will be from 9am to 3pm