The SCORE (Systematic Coronary Risk Evaluation) risk estimation system estimates the 10-year risk of death due to coronary or noncoronary cardiovascular disease (cardiovascular risk).1 The SCORE risk charts are easy to use because they include few parameters: age, sex, systolic blood pressure (SBP), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), and smoking. High cardiovascular risk is defined as a 10-year risk of 5% or higher. The guidelines of the fifth Joint Task Force of the European Societies on Cardiovascular Disease Prevention recommend use of the SCORE risk charts to calculate this risk.2
A limitation of the original SCORE risk chart is that it does not accurately calculate risk in individuals older than 65 years. The SCORE investigators recently published specific risk charts for people above this age threshold, using data from the original SCORE cohorts from Italy, Belgium, and Denmark and a new cohort from Norway.3
The aim of the present study was to evaluate the SCORE OP (SCORE Older Persons) risk charts in a Spanish population of people aged 65 years and above.
A cross-sectional study was undertaken in men and women aged 65 to 69 years attending 2 primary care centers. Study participants had at least 1 valid record of SBP and TC for the period 2010 to 2012 (when multiple readings were available, the most recent was selected). The study excluded individuals with a history of cardiovascular disease, as well as those with diabetes mellitus, because this disease is not included in the original SCORE risk calculations.
Cardiovascular risk was calculated according to the SCORE and SCORE OP risk charts for low-risk countries.1,3 In total, 17.56% of the study participants had no HDL-C values in their medical records; missing values were calculated by multiple imputation using chained equations according to Rubin's rules.4
Differences between men and women were evaluated using tests for independent data. Mean risk scores according to each SCORE chart were compared by calculating the intraclass correlation coefficient, and agreement between categorized risk levels was evaluated from the weighted kappa statistic. Data were analyzed with StataMP14 (StataCorp LP).
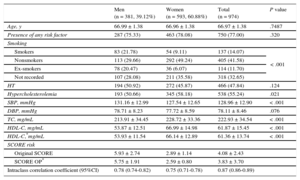
Data were analyzed from 974 patients aged 65 to 69 years whose cardiovascular risk could be calculated. General patient characteristics are presented in Table 1. The prevalence of smoking was higher among men, whereas a diagnosis of hypercholesterolemia was higher in women and was also associated with higher HDL-C levels. The overall intraclass correlation coefficient was 0.87 (95%CI, 0.86-0.89).
General Characteristics of the Patients Evaluated
| Men (n = 381, 39.12%) | Women (n = 593, 60.88%) | Total (n = 974) | P value | |
|---|---|---|---|---|
| Age, y | 66.99 ± 1.38 | 66.96 ± 1.38 | 66.97 ± 1.38 | .7487 |
| Presence of any risk factor | 287 (75.33) | 463 (78.08) | 750 (77.00) | .320 |
| Smoking | ||||
| Smokers | 83 (21.78) | 54 (9.11) | 137 (14.07) | < .001 |
| Nonsmokers | 113 (29.66) | 292 (49.24) | 405 (41.58) | |
| Ex-smokers | 78 (20.47) | 36 (6.07) | 114 (11.70) | |
| Not recorded | 107 (28.08) | 211 (35.58) | 318 (32.65) | |
| HT | 194 (50.92) | 272 (45.87) | 466 (47.84) | .124 |
| Hypercholesterolemia | 193 (50.66) | 345 (58.18) | 538 (55.24) | .021 |
| SBP, mmHg | 131.16 ± 12.99 | 127.54 ± 12.65 | 128.96 ± 12.90 | < .001 |
| DBP, mmHg | 78.71 ± 8.23 | 77.72 ± 8.59 | 78.11 ± 8.46 | .076 |
| TC, mg/mL | 213.91 ± 34.45 | 228.72 ± 33.36 | 222.93 ± 34.54 | < .001 |
| HDL-C, mg/mL | 53.87 ± 12.51 | 66.99 ± 14.98 | 61.87 ± 15.45 | < .001 |
| HDL-C,*mg/mL | 53.93 ± 11.54 | 66.14 ± 12.89 | 61.36 ± 13.74 | < .001 |
| SCORE risk | ||||
| Original SCORE | 5.93 ± 2.74 | 2.89 ± 1.14 | 4.08 ± 2.43 | |
| SCORE OP* | 5.75 ± 1.91 | 2.59 ± 0.80 | 3.83 ± 3.70 | |
| Intraclass correlation coefficient (95%CI) | 0.78 (0.74-0.82) | 0.75 (0.71-0.78) | 0.87 (0.86-0.89) |
DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; HT, hypertension; 95% CI, 95% confidence interval; SBP, systolic blood pressure; SCORE, Systematic Coronary Risk Evaluation; SCORE OP, Systematic Coronary Risk Evaluation Older Persons; TC, total cholesterol.
Data are expressed as no. (%) or mean ± standard deviation.
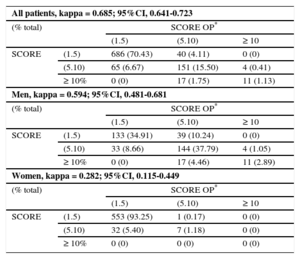
The kappa statistic revealed good agreement between the 2 cardiovascular risk scales overall (kappa = 0.685) and in men (kappa = 0.594), but agreement was weaker for women (kappa = 0.282). By comparison with the original SCORE chart, use of the SCORE OP chart moved 11.29% of men and 0.17% of women to a higher risk category and moved 13.12% of men and 5.4% of women to a lower risk category (Table 2).
Comparison of Risk Classification of Patients Aged 65 to 69 Years According to the SCORE and SCORE OP Risk Charts for Low-risk Countries
| All patients, kappa = 0.685; 95%CI, 0.641-0.723 | ||||
| (% total) | SCORE OP* | |||
| (1.5) | (5.10) | ≥ 10 | ||
| SCORE | (1.5) | 686 (70.43) | 40 (4.11) | 0 (0) |
| (5.10) | 65 (6.67) | 151 (15.50) | 4 (0.41) | |
| ≥ 10% | 0 (0) | 17 (1.75) | 11 (1.13) | |
| Men, kappa = 0.594; 95%CI, 0.481-0.681 | ||||
| (% total) | SCORE OP* | |||
| (1.5) | (5.10) | ≥ 10 | ||
| SCORE | (1.5) | 133 (34.91) | 39 (10.24) | 0 (0) |
| (5.10) | 33 (8.66) | 144 (37.79) | 4 (1.05) | |
| ≥ 10% | 0 (0) | 17 (4.46) | 11 (2.89) | |
| Women, kappa = 0.282; 95%CI, 0.115-0.449 | ||||
| (% total) | SCORE OP* | |||
| (1.5) | (5.10) | ≥ 10 | ||
| SCORE | (1.5) | 553 (93.25) | 1 (0.17) | 0 (0) |
| (5.10) | 32 (5.40) | 7 (1.18) | 0 (0) | |
| ≥ 10% | 0 (0) | 0 (0) | 0 (0) | |
CI95%, confidence interval 95%; SCORE, Systematic Coronary Risk Evaluation; SCORE OP, Systematic Coronary Risk Evaluation Older Persons.
Data are expressed as no. (%).
The 2 risk charts thus show a satisfactory level of agreement by intraclass correlation coefficient and kappa statistic (except for women); however, cardiovascular risk was systematically lower on the SCORE OP chart. European guidelines recommend a more cautious pharmacological approach with patients older than 60 years because the calculated risk can be high simply due to the patient's age, even when no other risk factors are present.
In Spain, 2 risk charts have been generated from direct analysis of the Spanish population, including the elderly population: the ERICE study, which includes participants ranging in age from 30 years to more than 80 years,5 and the FRESCO study, which includes individuals aged from 35 to 79 years.6 These risk calculations are awaiting external validation of their usefulness and impact compared with already available risk charts.
A limitation of the present study is the incomplete dataset for SBP and TC, which impeded risk calculation for some patients. Another limitation is that the analysis was restricted to primary care patients, raising uncertainties about whether the results can be extrapolated to the general population.
Among people older than 65 years, the SCORE OP risk chart gives lower cardiovascular risk estimates than the original SCORE chart, suggesting that fewer patients in this age group might benefit from statin therapy than previously thought. Further validation studies of these risk charts are needed in the Spanish population to assess the level of discrimination and calibration.
FUNDING15a Premi de Recerca, Fundació Mutuam Conviure.