To the Editor,
A 29-year-old woman was evaluated for a 2-month history of dyspnea and fatigue. Her medical history included an operation for hepatic cyst hydatid a year earlier. Chest radiography showed a well-defined paracardiac mass silhouette located near the left ventricle (Figure 1A, arrow). Echocardiography revealed noncalcified cystic lesion with internal septations at the junction of the left ventricle anterolateral segment extending to the cardiac apex without significant hemodynamic compromise (Figure 1B, arrow). Thoracic contrast magnetic resonance imaging (MRI) confirmed the presence of a well-defined, thin-walled cyst with T1 hypointense contents separated by hyperintense septae. The mass measured 10 x 10cm and had a wide attachment to the pericardium but caused no effusion (Fig. 1C, arrow). The cyst was approached through a left ventriculostomy and injected with hypertonic saline solution. The daughter cysts were then removed and the cyst wall was completely excised intrapericardially (Figure 1D). Postoperatively, the symptoms resolved and the patient received a 6-month course of 400mg twice a day of oral albendazole therapy. Follow-up echocardiography confirmed the absence of cyst contents in the heart.

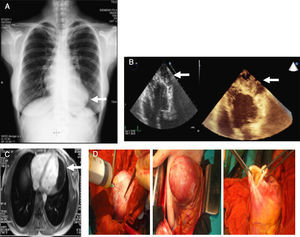
Figure 1. A, There is evident deformity of the cardiac silhouette near the left ventricle (arrow). B, Echocardiography showed cystic lesion at the junction of the left ventricle anterolateral segment extending to the cardiac apex (arrows). C, Cardiac magnetic resonance; an image of the cyst, had a wide attachment to the pericardium (arrow). D, Surgical resection of the cyst.
The incidence of cardiac involvement among patients with hydatid disease is 0.5% to 2%, and a pericardial site of implantation is even less common. Clinical development depends on the size, location, and integrity of the cyst, but in some cases it is asymptomatic1. Diagnosis can be difficult. It should be suspected from a chest radiography, which can easily detect deformities in the cardiac contour, as occurred in our case2. Echocardiography is the modality of choice for the diagnosis of cardiac hydatid cysts, owing to its widespread availability, high sensitivity, superior resolution, and the ability to analyze concurrent hemodynamic consequences. The multiloculated cystic nature of the lesion and presence of daughter cysts are well demonstrated on echocardiography. Multidetector computed tomography and MRI may aid in accurate localization of the lesion, detection of multiple lesions, study of concurrent lung lesions, and detection of multiorgan involvement, as well as differential diagnosis and follow-up.
Once the diagnosis of a hydatid cyst in the heart is made, immediate surgery is the treatment of option because of the potential risk of rupture and anaphylaxis. The cysts may also rupture into the pericardial cavity and cause pericardial effusion or tamponade and the formation of daughter cysts3. In our case, the patient was operated on and received medical treatment with an antiparasitic drug.
Corresponding author: maliastarcioglu@hotmail.com