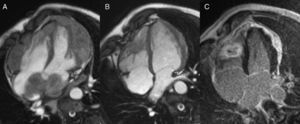
A 35-year-old man from Senegal was admitted for fatigue, shortness of breath, lumps in his skin, and lower back pain. Tuberculosis was diagnosed by tuberculin skin test and Mycobacterium tuberculosis was isolated from skin abscesses. Chest computed tomography revealed tubercular spondylodiscitis, while it excluded pulmonary involvement. Cardiac magnetic resonance showed a thick dysomogeneous pericardial mass infiltrating ventricular and atrial myocardium (Figure 1A). After a 6-month antibiotic therapy with isoniazid, rifampin and pyrazinamide, the patient reported substantial symptom improvement and cardiac magnetic resonance confirmed significant regression of the myopericardial masses. Only a right ventricular mass and a left ventricular epicardial thickening were still present (Figure 1B), both characterized by a dense fibrosis on gadolinium delayed enhancement imaging (Figure 1C). The right ventricular mass, in particular, presented a typical tubercular structure, with a fibrotic cap surrounding a necrotic core. Whereas tuberculous pericarditis has been reported in up to 1% of patients with active tuberculosis, myocardial involvement is very rare, sometimes causes hemodynamic compromise, thromboembolism or refractory arrhythmias, and may even require surgical treatment in addition to antibiotic chemotherapy.

Figure 1.
Corresponding author: barison@sssup.it