
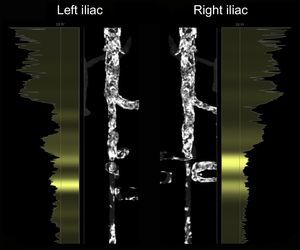

An 81 year-old male was referred for transcatheter aortic valve implantation (TAVI) because of a degenerated Carpentier Edwards Perimount 25mm (2005). He had a coronary artery bypass graft, involving a left internal mammary artery to the left anterior descending coronary artery and a saphenous vene to the posterior descending artery. Multidetector row computed tomography imaging showed iliac arteries with a lumen of 5.5-6.0mm and a tortuous course with severe calcifications (Figures 1 and 2). Due to the risk of vascular complications associated with a transfemoral access, the patient was accepted for a transapical TAVI using the JenaValve 23mm (JenaValve Technology GmbH, Germany).


During the procedure, we opened the sheath releasing the 3 “positioning feelers” of the JenaValve. Upon positioning, the clips were released impeding fixation of the device to the bioprosthesis (Figure 3A). We released the JenaValve in the ascending aorta where it remained rocking, potentially blocking the ostium of the brachiocephalic trunc. We performed a transfemoral rescue with a CoreValve bioprosthesis (Medtronic, United States). We advanced the CoreValve through the JenaValve without displacing it (Figure 3B). We then successfully deployed it in the bioprosthesis (Figure 3C).

After releasing the feelers, an automatic stop in the Cathlete Plus Delivery Systems prevents it from rotating further until the safety button is pushed. In this case, the clipping mechanism was prematurely released due to a faulty spring in the safety button mechanism. Because of similar cases, this lead to a temporary voluntarily recall of all Cathlete Plus Delivery Systems from the market in 2014.