Right atrial (RA) dissection is very rare. This is the first case of spontaneous RA dissection without rupture, which was successfully treated by surgery.
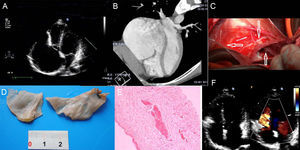
An 18-year-old man with no history of cardiac surgery or thoracic trauma presented to hospital with tachycardia and dyspnea. Chest roentgenogram demonstrated an enlarged heart. Transthoracic echocardiography revealed a significantly enlarged RA (11.3×7.7cm), normal left ventricular ejection fraction, and thickened tricuspid valve with deformation conglutinating with enlarged RA. Trivial regurgitation was present (Figure A). Computed tomography showed a significant enlargement of the RA and deformed right ventricular outlet and tricuspid annular (Figure B).

A presumptive diagnosis of Ebstain abnormality was made and surgery was performed with cardiopulmonary bypass. During the operation, the RA enlarged significantly and the wall was paper thin. The anterior wall of the RA dissected and the area was about 3×4cm. The right coronary artery could be seen in the muscle. The tricuspid annulus was enlarged with normal tricuspid valve (Figure C). The thin atrial wall was dissected and autogenous pericardium was immobilized between the muscle and tunica adventitia of the RA with 6/0 Prolene. Tricuspid valvuloplasty was performed with the autogenous pericardial strip and no regurgitation with water injection test. The histopathological examination showed that the atrial wall consisted of fibrin with fractured elastic fiber and several residual degenerative myocardial tissues (Figures D and E). During follow-up, echocardiography showed a normal RA without residual dissection and no tricuspid insufficiency (Figure F). Right atrial dissection is a rare entity and its diagnosis poses a challenge even when the best imaging techniques are applied. Only surgical exploration can clarify the reason for the enlarged RA.