To the Editor,
Both genetic and environmental factors are involved in the development of coronary disease (CD). The degree to which each particular risk factor contributes to the development of CD is not precisely known; in particular, the role of genetics, beyond its indirect role through the hereditary component of hypercholesterolemia, is still not clear. Twin studies could be helpful in researching the role of genetics in the development of CD.1
We describe 2 identical twins diagnosed with unstable angina, in both cases with right coronary artery disease, within an interval of 6 months, and both treated percutaneously with placement of a coronary stent.
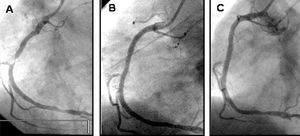
The first case is a 49-year-old man who presented hypertension, smoking, and dyslipidemia as cardiovascular risk factors. The patient, who had no history of heart disease, was hospitalized with clinical symptoms of unstable angina, associated with T-wave negativity on the inferior aspect. Cardiac catheterization disclosed severe stenosis in the proximal segment of the right coronary artery (Figure 1A), with no significant angiographic stenosis in the remaining arteries. An ad hoc percutaneous coronary intervention was performed, with direct implantation of a 4x28-mm Taxus stent (Boston Sci), with good angiographic results and no complications (Figure 1B). At 6 months the patient was clinically asymptomatic and angiographic follow-up showed no restenosis (Figure 1C).

Figure 1. A: severe stenosis in the proximal segment of the right coronary artery. B: immediate direct postimplantation of a 4x28-mm Taxus stent. C: angiographic control at 6 months' follow-up.
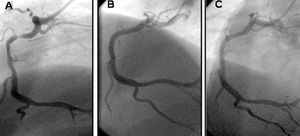
Six months after this patient was admitted, his identical twin brother (age 49) was hospitalized with symptoms of progressive angina. The patient presented the same cardiovascular risk factors (hypertension, smoking, and hyperlipidemia). The baseline electrocardiogram showed no specific repolarization abnormalities. Coronary angiography showed a severe lesion in the middle right coronary artery, but no significant lesions in the remaining coronary vasculature (Figure 2A). As occurred with the patient's brother, the right coronary artery was treated, in this case with a 4x15-mm bare metal stent (Driver, Medtronic Inc.) (Figure 2B). After six months' follow-up, this patient remained asymptomatic, with no restenosis in follow-up angiography (Figure 2C).

Figure 2. A: severe lesion in the middle right coronary artery. B: immediate direct postimplantation of a 4x15-mm Driver stent. C: angiographic control at 6 months' follow-up.
The earliest cardiologic studies in twins consisted of electrocardiogram analysis in 1925. By the late 20th century, studies have focused on CD, with considerable attention and debate regarding the genetic versus environmental factors in the pathogenesis of this condition.
It has been shown that twins are closely matched in terms of CD, although this effect decreases with age. It is estimated, for example, that the probability of dying due to CD in the next 10 years is 50% for a 55-year-old man if his twin has had a myocardial infarction.2 In 1958, Benedict3 described a set of twins with CD. His report mentioned several points of interest: young age (40 years), similar electrocardiogram changes, and development of coronary events with a small difference in time (6 months). At that time, this report was considered an argument in favor of the role of hereditary factors on the development of CD.2,3 For example, a later study reported on a set of 50-year-old twins who presented with an acute coronary syndrome two years apart; one had an infarction and the other angina, but the location and characteristics of the coronary lesions were similar. It was considered that a high index of suspicion of occult CD should be maintained in the asymptomatic twin if a coronary event has occurred in the other twin.2
In terms of coronary angiography, little is known about angiographic expression of CD in twins.4,5 In some cases, the location of the CD was similar in both twins. In contrast, other authors mention that, despite the similarity in risk factors, there may be important differences in both the anatomy and the degree of CD in identical twins.2,4 The 2 patients we present had lesions in the same location (right coronary artery) and, curiously, the procedures were performed by the same professional (RM).
Unlike Mendelian genetics, cardiac diseases may represent a more complex association of genes that modify the course of the disease, with environmental influences as risk factors. In any case, the patients we describe illustrate the genetic component in the pathogenesis of CD and, at least, confirm the value of establishing a high degree of suspicion of CD in a twin once CD has been documented in the other.