We thank Moreno-Martínez et al for their comments regarding our letter.1 As they mention, the incidence of dual left anterior descending artery in healthy hearts is approximately 1%. Although the true incidence of descending septal artery based on coronary angiographic findings is unknown, its presence has been detected in a surprisingly high percentage of postmortem studies. Rodríguez et al2 identified the descending septal artery in 12% of 427 specimens; Taylor,3 in 68% of 112; and Sahni and Jit,4 in 85% of 500 autopsy subjects. As we stated in the above-mentioned letter, this could be explained by the high perfusion pressures used during these studies (reaching 280mmHg) and the loss of muscle tone, or by the absence of surrounding tissue, which would facilitate the visualization of this vessel.5
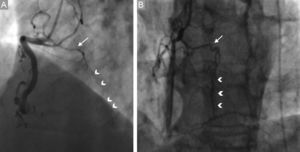
This high detection rate, in contrast to the 1% reported for dual left anterior descending artery, could indicate that the descending septal artery is an anatomical variant that is underdetected by conventional angiography, rather than a coronary artery anomaly per se. Its development appears to be more evident in the presence of obstructive coronary artery disease,5 suggesting the “recruitment” of descending septal artery as a source of collateral circulation (Figure).
, which provides homocoronary collateral circulation (arrow heads) toward distal right coronary artery in the presence of an acute occlusion (A) and chronic occlusion (B) of right coronary artery.")
We agree with Moreno-Martínez et al in the need for an adequate assessment of the descending septal artery, taking into account its potential role in certain clinical scenarios.