

Keywords
INTRODUCTION
Myocarditis is an acute or chronic inflammatory process that affects the myocardium in response to the action of various infectious, chemical or physical agents. In most patients the disease is self-limiting. The natural course of myocarditis varies greatly, ranging from an asymptomatic state secondary to local inflammation, through development of dilated cardiomyopathy with a variable course, to fatal heart failure due to disseminated myocarditis. The diagnosis of myocarditis during an acute episode may prove difficult, due to the lack of diagnostic techniques with acceptable degrees of specificity and sensitivity. Although endomyocardial biopsy is still considered the diagnostic gold standard, the development of new imaging techniques, such as cardiac magnetic resonance imaging (MRI), have contributed greatly to the diagnosis of myocarditis.
CASE REPORT
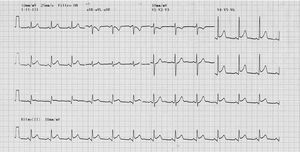
We present the case of a 39-year old man, who apart from smoking five cigarettes a day, had no other cardiovascular risk factors. The patient presented to the emergency department with a 6-hour history of oppressive central chest pain with typical characteristics but no disturbances of the vegetative nervous system. The blood pressure was 110/70 mm Hg, the heart rate 82 bpm, and cardiac auscultation revealed a fourth heart sound; the remainder of the examination was unremarkable. An electrocardiogram (Figure 1) showed ST segment elevation of 2 mm in the inferior, posterior and lateral leads, and the patient was admitted to the Intensive Care Unit with a suspected acute, inferolateral myocardial infarction.

Figure 1. 12-lead electrocardiogram showing ST segment elevation of 2 mm in leads II, III, aVF, V4, V5, and V6.
After admission to the Intensive Care Unit, antiplatelet aggregation therapy was given and thrombolysis was performed with TNK. No electrocardiographic changes were detected over the subsequent hours, although there was slight improvement in the pain, and a peak creatine kinase enzyme of 1014 and its MB isoenzyme of 110 nine hours after thrombolysis. Hematologic, hemostatic, biochemical, and kidney function values were all normal. Sixteen hours after admission, because of the persistent ST segment elevation, contrast-enhanced echocardiography was done, showing preserved overall left ventricular function, with inferior, posterior and lateral hypokinesia, with no valvular alterations. Coronary arteriography showed angiographically normal coronary arteries.
The patient was later transferred to the ward where, with bed rest, his clinical condition improved satisfactorily. Serologic tests for enterovirus, herpesvirus, cytomegalovirus and atypical bacteria were all negative.
Gadolinium enhanced cardiac MRI (Siemens Symphony) showed delayed uptake of contrast with a subepicardial and intramyocardial patchy pattern that respected the subendocardium and was localized to the posterior and lateral regions, with posterobasal hypokinesia, highly suggestive of myocarditis (Figures 2 and 3).

Figure 2. Cardiac magnetic resonance image obtained by inversion recovery gradient echo sequence (Turbo Flash) (Siemens Symphony). Inlet-outlet plane of the left ventricle. Image obtained 10 min after injection of gadolinium. The arrows indicate the patchy pattern of intramyocardial uptake of gadolinium.

Figure 3. Magnetic resonance image obtained by inversion recovery gradient echo sequence (Turbo Flash) (Siemens Symphony). Short axis. The arrows indicate the subepicardial uptake of gadolinium in the posterolateral region.
The patient was discharged five days later with no symptoms. An electrocardiogram (ECG) showed discrete ST segment elevation in the same leads as before. At follow-up examination three weeks later, the patient was still asymptomatic, the ECG showed T wave inversion in the inferior and lower lateral wall and echocardiography showed normal regional contractility.
DISCUSSION
The diagnosis of acute myocarditis is often difficult. ST segment elevation together with an increase in markers of myocardial damage in a patient with central chest pain may suggest a possible acute, transmural myocardial infarction. The patient reported herein had symptoms highly suggestive of myocardial ischemia and the rise in enzymes followed a typical curve, with no isolated or intermittent increase in the creatine kinase, as is usual in myocarditis.
The absence of mirror image changes in the ST segment on the ECG, as noted on the ECG of our patient, is a finding that may help to establish a diagnostic suspicion of myocarditis.
The rise in markers of myocardial damage in our patient, as well as the ECG changes, were interpreted as an acute coronary syndrome with ST segment elevation, and it was decided to undertake reperfusion therapy. Coronary angiography, performed 16 hours after admission because of the persistent ST segment elevation and alterations in regional contractility on the echocardiogram, showed angiographically normal coronary vessels. A diagnosis of very probable myocarditis was therefore made.
The difficulty in diagnosing myocarditis lies in the known absence of specificity and sensitivity of the various diagnostic techniques used. Systematic biochemical measurements are not diagnostic and an increase in cardiotropic virus antibodies only reflects the response to a recent viral infection, but does not indicate active myocarditis. Endomyocardial biopsy, considered to be the diagnostic gold standard, is associated with a not inconsiderable risk of disease, as well as with sampling errors due to the focal involvement of the myocardium, which therefore reduces its diagnostic sensitivity. Radioactive isotope studies, widely used for the diagnosis of myocarditis, are limited by their low specificity, the exposure to radiation, and their cost.
Several studies have been published over recent years concerning the use of delayed contrast-enhanced cardiac MRI as a diagnostic technique in patients with a high clinical suspicion of myocarditis. Cardiac MRI shows the accumulation of contrast in the myocardium as a consequence of the breakdown of the myocyte membrane resulting from the inflammatory process.1 The uptake of contrast usually has a characteristic patchy pattern for about the first 2 weeks after the acute event, later becoming progressively more disseminated, as seen by Friedrich et al in 16 of 19 patients with viral myocarditis.2,3 Moreover, this pattern of contrast uptake is easily distinguished from the subendocardial pattern of uptake seen in acute myocardial infarction.4,5 Roditi et al,6 as well as noting focal enhancement of gadolinium in involved areas, also established by cine-MRI that the association of changes in regional contractility in the areas of uptake considerably increased the degree of diagnostic accuracy.6 Mahroldt et al7 recently reported a clear association between the focal uptake of contrast and histopathologically determined foci of active myocarditis.
Cardiac MRI with contrast in association with cine-MRI is a useful tool for the diagnosis of myocarditis and provides an alternative to endomyocardial biopsy. The focal uptake of subepicardial contrast associated with regional changes in contractility are reliable indicators of areas of active myocarditis, as reported in recent studies. The availability of this diagnostic technique in the context of an acute episode might obviate the use of other, invasive diagnostic techniques which are not exempt from associated disease.
Correspondence: Dr. A. Subinas Elorriaga.
Jon de Arróspide 26, 7.o C. 48014. Bilbao. Vizcaya. España.
E-mail: al.subinas@euskalnet.net